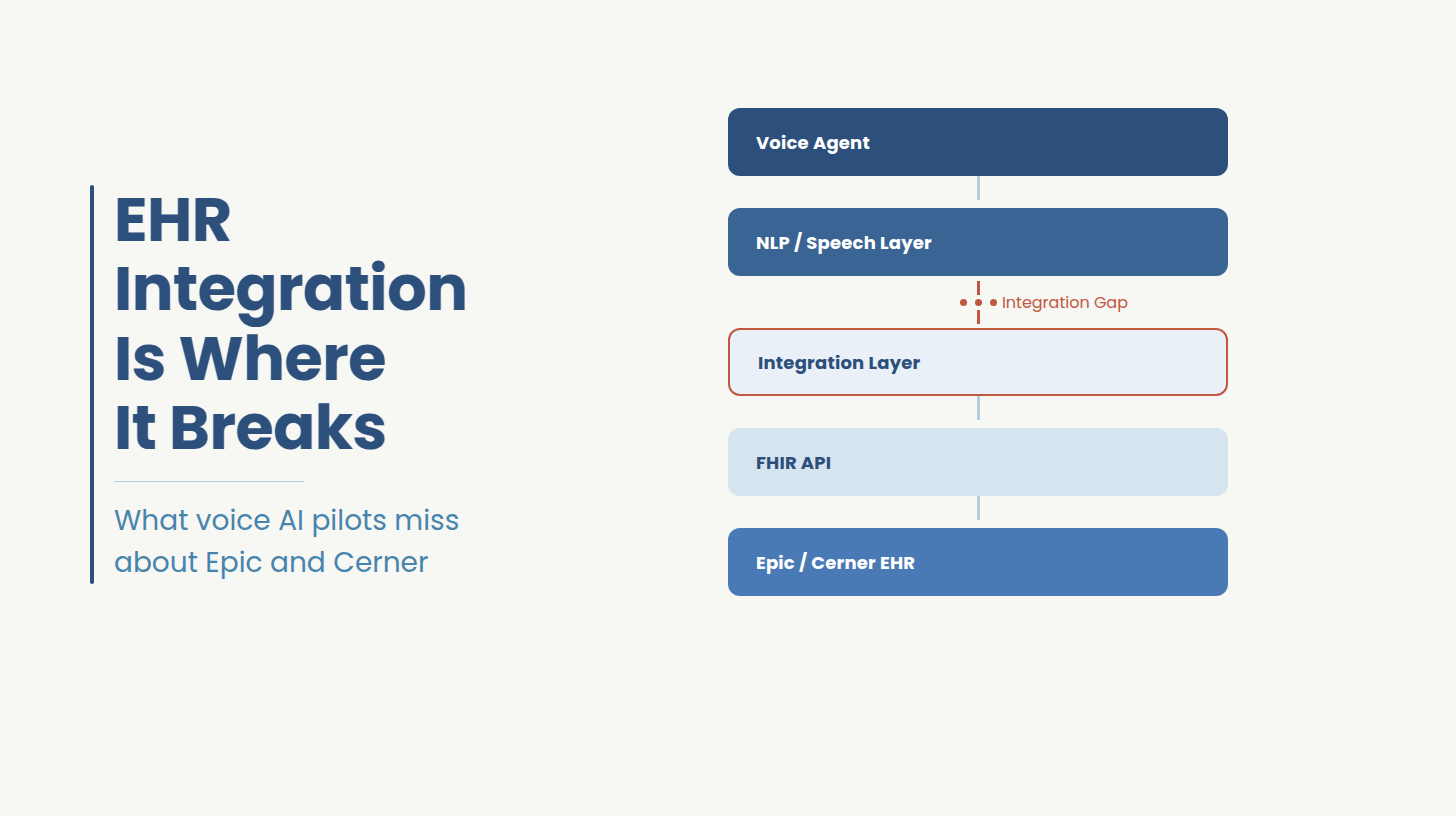
AI voice agents for healthcare are handling scheduling calls, capturing patient intake information, collecting insurance details, and routing inquiries without a live agent on the line. Whether any of that actually works, from the patient's perspective and from the clinical operations team's perspective, depends almost entirely on how the voice agent connects to the EHR. Conversational AI in healthcare has matured enough that the speech and NLP layers are reliable. The integration layer is where deployments succeed or fail. This blog covers why EHR integration is consistently the hardest part of any voice agent deployment, and what it takes to get it right in Epic and Cerner environments.
A regional health system finished a voice AI pilot with numbers that looked good on paper. Call containment was up yet live agent transfers were down. The project was greenlit for full deployment.
Three months in, clinical operations raised a flag. Appointment no-shows had not moved. Front desk staff were still manually entering intake data after every shift. Patients were calling back about appointments the system had confirmed but never actually booked in Epic.
The voice technology had worked exactly as designed. The integration into Epic had not. The engineers working on it had never been inside that health system's specific Epic configuration before.
As of 2021, 96% of non-federal acute care hospitals in the U.S. run on a certified EHR system.[1] Epic and Cerner together account for the majority of that installed base, with environments that have accumulated a decade or more of custom configuration. Conversational AI in healthcare can be deployed quickly at the voice layer. The EHR layer cannot be shortcut.
An integration built against the FHIR specification will fail against your instance the first time it hits one of those specifics. Most voice AI vendors know this. Their response is a professional services engagement handed to a team that has never been inside your Epic environment, working from documentation your EHR team produces during the project. That documentation reflects what the team remembers, not what actually exists.
A voice agent that completes clinical workflows needs these four things built against your specific environment, not a reference implementation.
The agent must read available appointment times at the moment of the call. Epic's $find operation and Cerner's Slot resource both support live queries.[2] A cache-based implementation confirms appointments against slots that no longer exist vs the slot was taken by a patient portal booking or a provider schedule change between the cache refresh and the call. When the write fails, the patient gets a confirmation the EHR does not honor. Your front desk absorbs the difference.
The FHIR scopes granted to the integration's service account determine what it can write and not what the voice layer is capable of doing. Without the correct Appointment.write, Patient.write, or Coverage.write scopes authorized by your Epic or Cerner team, the agent completes calls and fails writes silently.[3] Scope authorization is not a formality. It is the step that determines what the system is actually allowed to do inside your EHR, and it requires direct coordination with your EHR team before development begins, not after.
A voice agent runs continuously without a user session. Patient-facing SMART tokens expire between sessions and require manual re-authorization.[4] On a system handling hundreds of calls per day, that expiry is a recurring production outage on a schedule. SMART on FHIR Backend Services handles server-to-server authentication using JWT-signed client assertions registered directly against your EHR's authorization server, so the integration maintains a valid session without human intervention. Getting this configuration wrong means either a system that re-authenticates manually on a cycle, or a security architecture your compliance team cannot sign off on.
Chief complaint, insurance details, and reason for visit each map to specific FHIR resources in your organizational configuration, not the generic specification. Chief complaint may map to Condition or Observation depending on how your clinical team configured the EHR. Insurance maps to Coverage. An integration built without validating these targets against your instance produces data the EHR rejects outright or stores in a location your staff cannot locate. The call is automated. The data entry is not.
Both platforms use FHIR R4 and SMART on FHIR. The similarity ends there.[5]
An integration team that has only built against Epic will need to relearn enough of the Cerner authorization model that a Cerner deployment should be scoped and timed independently. Do not assume the work transfers.
A health system in the southeast assumed their voice AI vendor's HIPAA compliance covered the full integration. They had the BAA. They had the vendor's SOC 2 report. What their compliance team found during an internal audit was different: call transcripts were being retained by a third-party speech model not named in the BAA, audit logs did not capture the full session state required for breach investigation, and PHI was being passed to the LLM in-context rather than through a de-identified input layer. None of this was visible in the vendor's compliance documentation. All of it was introduced at the integration layer.[6]
Zero data retention from an LLM provider addresses the PHI-in-context question partially. SOC 2 Type II from the voice vendor confirms their internal controls. Neither covers your integration's data handling. The compliance work that matters happens during integration architecture design, not after deployment.
Get a Free Scoping Session for Your EHR Voice Agent Integration
If your voice agent is selected and the EHR integration is the current blocker scope authorization not confirmed, slot discovery not validated against your instance, write-back not tested against your Epic or Cerner configuration that is exactly what this session is for.
In 30 minutes, Ideas2IT reviews your integration requirements and delivers a project plan with a defined scope of work, a timeline, and a cost estimate your team can take to procurement.
Book a 30-minute scoping call →
The failure is almost never a technology failure. It is an environment mismatch. The integration was built against a reference environment. Production surfaces the differences.
Both root causes trace to the same decision: the integration was treated as a configuration step at the end of a product deployment, not as an engineering project with its own environment-specific complexity.
Most health system engineering teams have deep EHR knowledge. What they typically do not have is experience building FHIR-native integrations for systems that run continuously, handle write-back under failure conditions, and extend across departments without a rebuild. That is a different skill set.
The question is not about headcount. It is about whether the engineers on your integration have solved this class of problem in a production environment before, or whether your deployment is where they learn it.
This is a risk question, not a capability question. Your in-house team can build this. The question is whether they have the specific production experience to build it without the learning curve arriving in your Epic environment.
Health systems that have run a voice AI pilot already know which failure pattern they hit first. The decision to bring in a partner is usually made after the first production failure, not before it. The cost of the first failure in staff time, patient complaints, and re-scoping typically exceeds the cost of the partner engagement that would have prevented it.
A multi-site health system brought Ideas2IT in after an initial voice AI deployment failed to reduce front desk call volume as projected. The voice layer was performing. The Epic integration was not writing back correctly: slot discovery was running against cached data, write-back scopes had not been fully authorized, and intake fields were not mapping to the resource structure the EHR expected.
Ideas2IT's Forward Deployed Engineers worked inside the health system's Epic sandbox from week one. The integration was rebuilt with live $find queries replacing the cached slot layer, correct write-back scope authorization confirmed with the health system's Epic team, and a resource mapping layer validated against the organization's actual clinical configuration rather than the generic FHIR specification.
Within 90 days of go-live on the rebuilt integration, the health system saw measurable improvements across front desk call volume for scheduling, appointment booking completion rates in the EHR, and manual data entry per shift for voice-originated appointments.
Ideas2IT is a platform-led AI and software engineering company with 800+ engineers, founded in 2009, and operating with a 99% client renewal rate. AWS GenAI Specialist Partner, SOC 2 Type II certified, ISO 27001 certified, AWS Healthcare Competency holder, and HIPAA-compliant across all delivery environments. That is the credential set of our healthcare software development offering. What health systems actually choose Ideas2IT for is the delivery model.
For the broader picture of what we build across EHR workflows, RPM, prior auth, and clinical decision support, check our healthcare use case page.
Ideas2IT deploys a Forward Deployed Pod inside your environment from day one, your Epic or Cerner instance, your security architecture, your integration standards, your standups, your OKRs. The pod is operational within two weeks and structured as follows:
FDEs work as senior team members with full business context, instead of as contractors executing a statement of work from the outside. An FDE working in your sandbox sees your slot rule structure, your granted scope set, and your existing integration dependencies. A remote team working from your documentation sees what the documentation says.
Every engagement runs on a purpose-built platform stack. For EHR voice agent integration, this directly compresses the highest-cost phases of the project:
Each platform encodes prior delivery experience. Teams are not solving the same class of problems from scratch. The result is 40–70% faster delivery than a conventional engineering team, with engineers working only on the 20–30% of the project that requires human judgment.
Every Ideas2IT engagement runs with weekly output visibility, sprint cadences, and structured handoff at every milestone. Every engagement ends with your team owning what was built embedded documentation, structured handoff protocols, and training so your team can maintain, extend, and scale the integration independently.
The engagement starts with a free 30-minute scoping call. Ideas2IT reviews your EHR integration requirements and delivers a project plan with a defined scope of work, a timeline, and a cost estimate before any development begins
Your voice agent should complete workflows
If the EHR integration layer is not right, everything else is call deflection with extra steps. Book a 30-minute scoping call with Ideas2IT's healthcare integration team. We review your Epic or Cerner environment, identify the specific gaps between your current integration state and what full workflow completion requires, and deliver a project plan with timeline and cost before any development begins.
Book a 30-minute scoping call →