Custom medical imaging software development is the process of building a health system's imaging infrastructure, AI integration layer, and clinical data architecture to its own specifications, rather than operating inside a PACS vendor's proprietary platform. The result is a system the health system owns, controls, and can extend without vendor permission.
The AI pilot ran clean and the data pipeline held. The radiology team approved the read accuracy. Then the PACS vendor's integration team quoted eighteen months.
The vendor in question is one of the larger names in enterprise PACS who is well-resourced, commercially active, with a published AI roadmap and a cloud migration program. The problem is their business model. The integration endpoint the health system needed required a modification to the vendor's proprietary API layer. That modification sat in a prioritization queue alongside requests from every other customer in their install base. Eighteen months was the honest answer.
Over 60% of U.S. hospitals are running at least one critical application on legacy software that lacks modern APIs or HL7 FHIR compatibility, according to a 2024 HIMSS Analytics study [3]. Most of those hospitals did not discover this during procurement. They discovered it when they tried to build past the system's boundaries when an AI initiative, a data science program, or a new payer contract requirement ran into an integration wall that could only be resolved by the vendor, on the vendor's schedule.
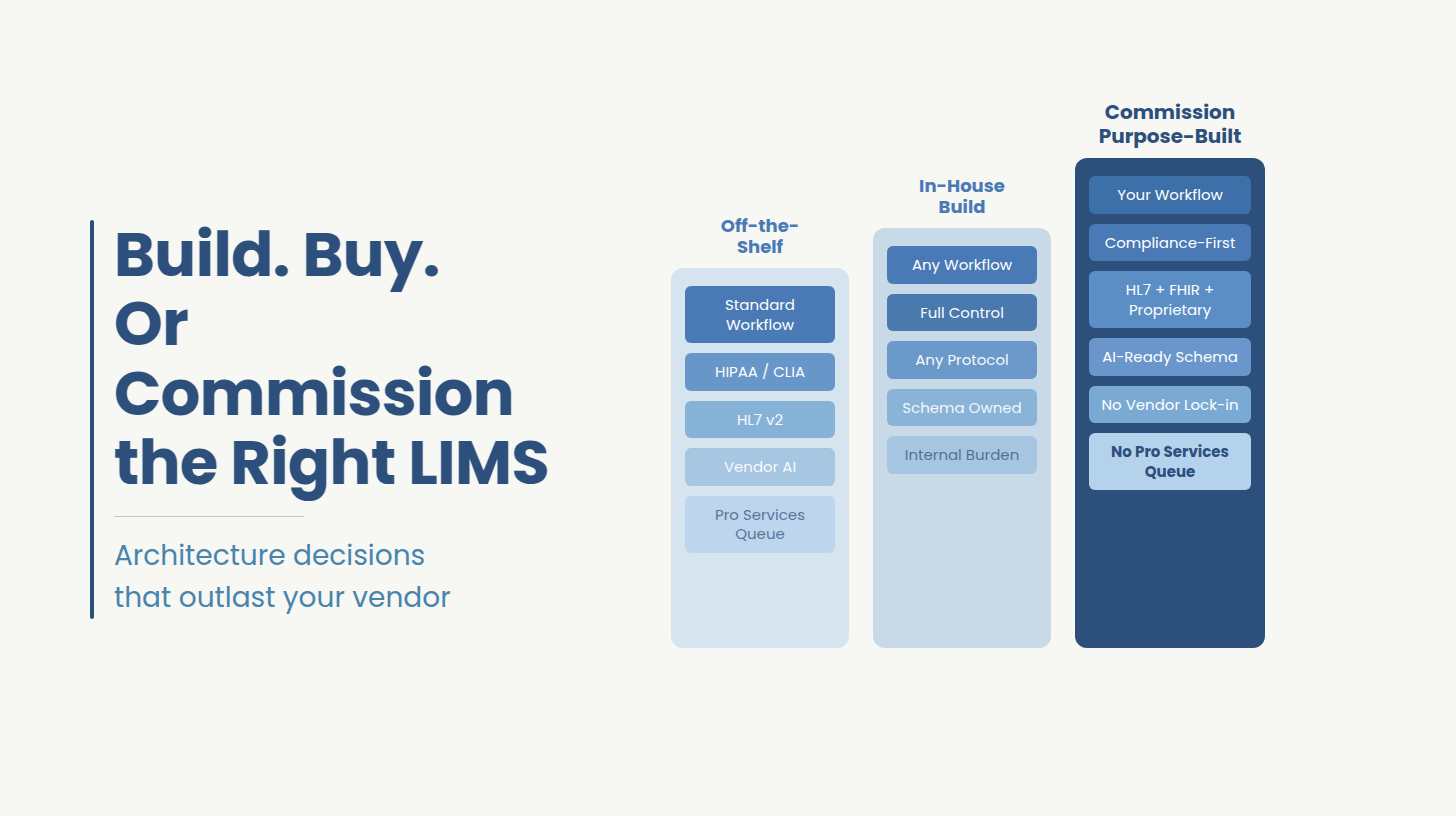
The decision most CTOs frame as "build vs buy" is not about a feature comparison or a cost calculation. It is a question about architecture ownership specifically, about who controls the integration layer between imaging data and the clinical programs that depend on it. Get that question wrong, and no amount of renegotiation fixes the answer.
The architecture of a traditional PACS is built around proprietary integration. The vendor controls the API layer, the storage format, the DICOM extensions, and the pathways through which external systems, AI tools, EHR platforms, data warehouses connect to the imaging stack. Proprietary integration is how PACS vendors create switching costs, protect renewal rates, and generate recurring revenue from the support contracts, data migration fees, and middleware layers that accumulate over a system's lifetime.
When a health system selects an AI diagnostic tool, the integration path for that tool runs through the PACS vendor's architecture. If the vendor has a pre-certified integration with that AI tool, deployment is possible on the vendor's timeline, through the vendor's support process. If the vendor does not, the health system faces a roadmap request, a custom engagement quote, or a flat refusal. The clinical performance of the AI tool is now based on the vendor's integration catalog.
The per-study fee model compounds this problem. AI-assisted diagnostics typically increase imaging utilization. Faster reads enable more studies, earlier detection drives follow-up imaging, and expanded access brings volume that would previously have been deferred. In a per-study fee structure, every incremental study is revenue for the PACS vendor. The health system is commercially incentivizing the vendor to grow the same volume base it is being charged to access. This is a structural misalignment built into the contract.
A third mechanism deserves attention, because it is where the most expensive mistakes are made. When a health system moves its legacy PACS to a cloud host and describes the result as a cloud migration, it has moved the infrastructure without changing the architecture. A cloud-enabled PACS carries the performance ceiling and vendor dependency of its original on-premise design regardless of where the servers physically sit. The proprietary integration layer, the roadmap dependency, and the per-study fee model all travel with it. A cloud-native PACS, built from the ground up on microservices with an open API architecture, is a genuinely different system. The two are not equivalent, and conflating them is the single most common planning error in enterprise imaging modernization.
The cost of staying inside this architecture accumulates quietly. Piedmont Healthcare saved more than $700,000 after implementing a vendor-neutral archive and moving away from a proprietary PACS model, with an additional $2 million in projected savings as further systems transitioned [9]. Children's Hospital of Philadelphia reported nearly $3 million in savings over five years through a similar structural exit [10]. These are not anomalies. They are the predictable result of removing a recurring cost structure that compounds with every contract renewal, every storage upgrade, and every integration request that has to go through a vendor queue.
The three mechanisms described above like proprietary integration architecture, per-study fee misalignment, and cloud-enabled systems carrying the constraints of their original on-premise design share a common structural effect. They make the vendor's release schedule the hard limit on a health system's clinical and technical ambitions. That limit has a name.
The Roadmap Ceiling is the point at which a PACS vendor's internal prioritization becomes the binding constraint on a health system's AI and integration programs not technical feasibility, not engineering capacity, not budget, but the vendor's release calendar.
This is worth stating carefully, because the argument is not that PACS vendors are failing their customers. The major enterprise PACS platforms have made genuine architectural progress over the past five years. Cloud-native offerings have emerged. Open API frameworks are more common than they were. AI orchestration layers are appearing in vendor roadmaps. The issue is not vendor quality. It is vendor control. Even a well-designed, well-resourced PACS vendor's roadmap is a roadmap the health system does not set, does not control, and cannot accelerate when a clinical or regulatory deadline requires it. The ceiling applies regardless of which vendor is in the data center.
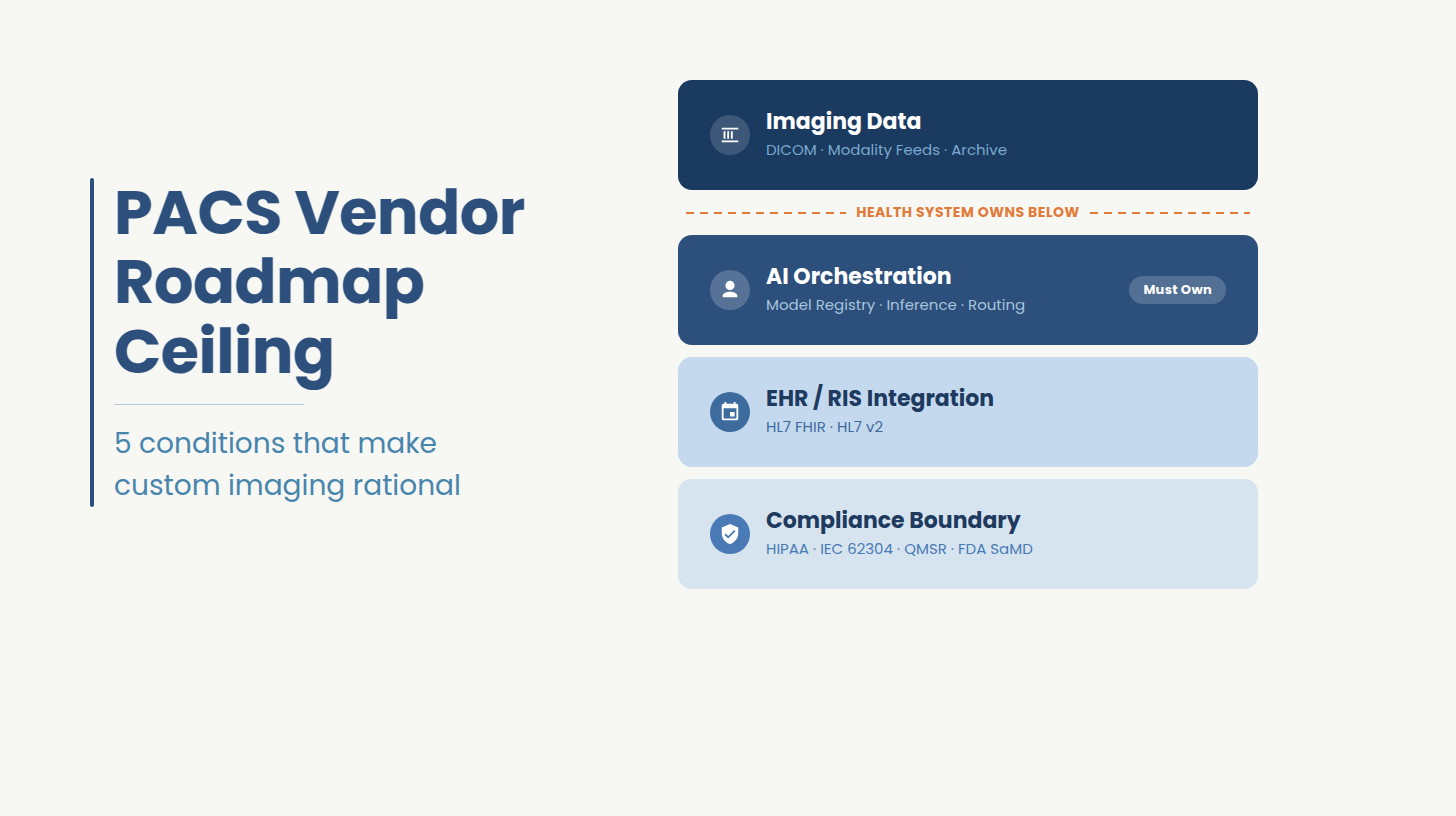
The build vs buy decision in medical imaging is not answered by a feature comparison. It is answered by measuring the current architecture against five specific conditions. The five conditions below form a diagnostic framework that converts the Roadmap Ceiling from an abstract concept into a set of yes-or-no tests against the current environment. If one applies, custom build deserves serious evaluation. If two or more apply, staying inside a proprietary PACS architecture is the higher-risk choice.
A hospital should evaluate custom medical imaging software development when one or more of the following conditions is present in its current environment. Each condition is diagnosable without a vendor engagement. If two or more apply, staying inside a proprietary PACS architecture carries more execution risk than a custom build.
The radiology AI market has matured at the specialty level. The leading stroke detection tool, the leading lung nodule tool, and the leading cardiac imaging tool are unlikely to come from the same vendor. When the PACS integration architecture is proprietary, a health system can only deploy the AI tools the PACS vendor has pre-certified or built an integration path for. Clinical performance stops being the selection criterion. The vendor's integration catalog becomes the selection criterion. A health system in this position is not choosing AI. It is choosing from a pre-approved list.
In an open-architecture or custom-built imaging platform, adding an integration endpoint is a sprint task. In a proprietary PACS, it is a roadmap request that enters a vendor prioritization queue, is evaluated against the vendor's commercial interests, and emerges on a timeline the health system does not set. The diagnostic question is simple: if the data science team needed a new data access pathway from the imaging stack today, would the first call go to an engineer or to a vendor account manager? If the answer is the account manager, the Roadmap Ceiling is already in place.
AI-assisted diagnostics increase imaging utilization. Faster reads enable more studies. Earlier detection drives follow-up imaging. Expanded access brings volume that would previously have been deferred or missed. In a per-study fee model, every study that the AI program generates is additional revenue for the PACS vendor. The health system is building a clinical program that commercially benefits its infrastructure vendor at a rate proportional to the program's success. That misalignment compounds with every percentage point of volume growth the AI initiative produces.
A health system's imaging data belongs to the health system. In practice, when that data lives inside a proprietary PACS archive in a vendor-specific format, accessing it for model training, population health analysis, or real-time AI inference requires engaging the vendor's support process or purchasing an additional data access tier. The data is inside the building. The team that needs it cannot reach it without vendor permission. Data ownership that requires vendor approval to exercise is not data ownership.
FDA's January 2025 draft guidance on AI-enabled device software lifecycle management introduced documentation and governance requirements that apply across the development, deployment, and post-market monitoring of any AI-integrated imaging system [7]. The February 2, 2026 enforcement of the QMSR aligning the FDA's Quality System Regulation with ISO 13485 extended those requirements to quality management systems across the device software lifecycle [8]. State-level data residency mandates and payer contract requirements around protected health information handling are adding further constraints on top of federal standards. When a health system's current PACS vendor cannot meet these requirements without a custom engagement priced comparably to a rebuild, the compliance trigger has been reached. The exit is now a requirement.
Working Session
If any of the five conditions above describes your current imaging environment, the problem is architectural rather than contractual. Renegotiating the current PACS agreement does not change the integration model. Switching to a different PACS vendor that operates the same proprietary architecture does not resolve it either.
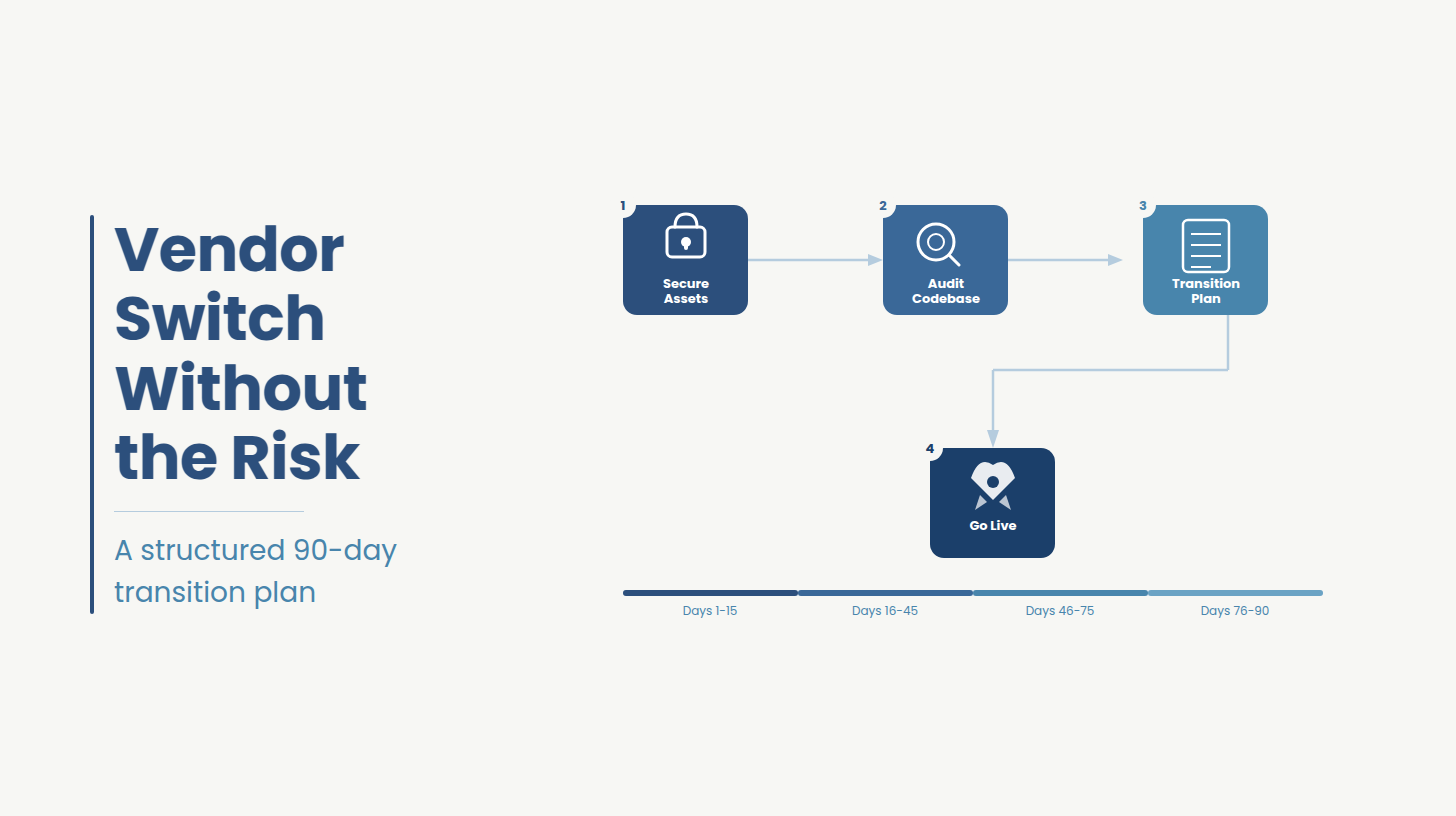
What the situation requires is a structured assessment of the current stack: where the Roadmap Ceiling sits, which of the three exit paths (modernize, replace, or build custom) is appropriate given the existing codebase, compliance requirements, and AI roadmap, and what each path costs and takes to execute.
Ideas2IT's healthcare engineering team runs exactly that assessment as a scoped, zero-cost engagement. A senior engineer and a compliance specialist review the current imaging stack, map the dependency between the PACS integration layer and the AI program, and deliver a written recommendation with cost and timeline ranges across all three paths.
Book the assessment
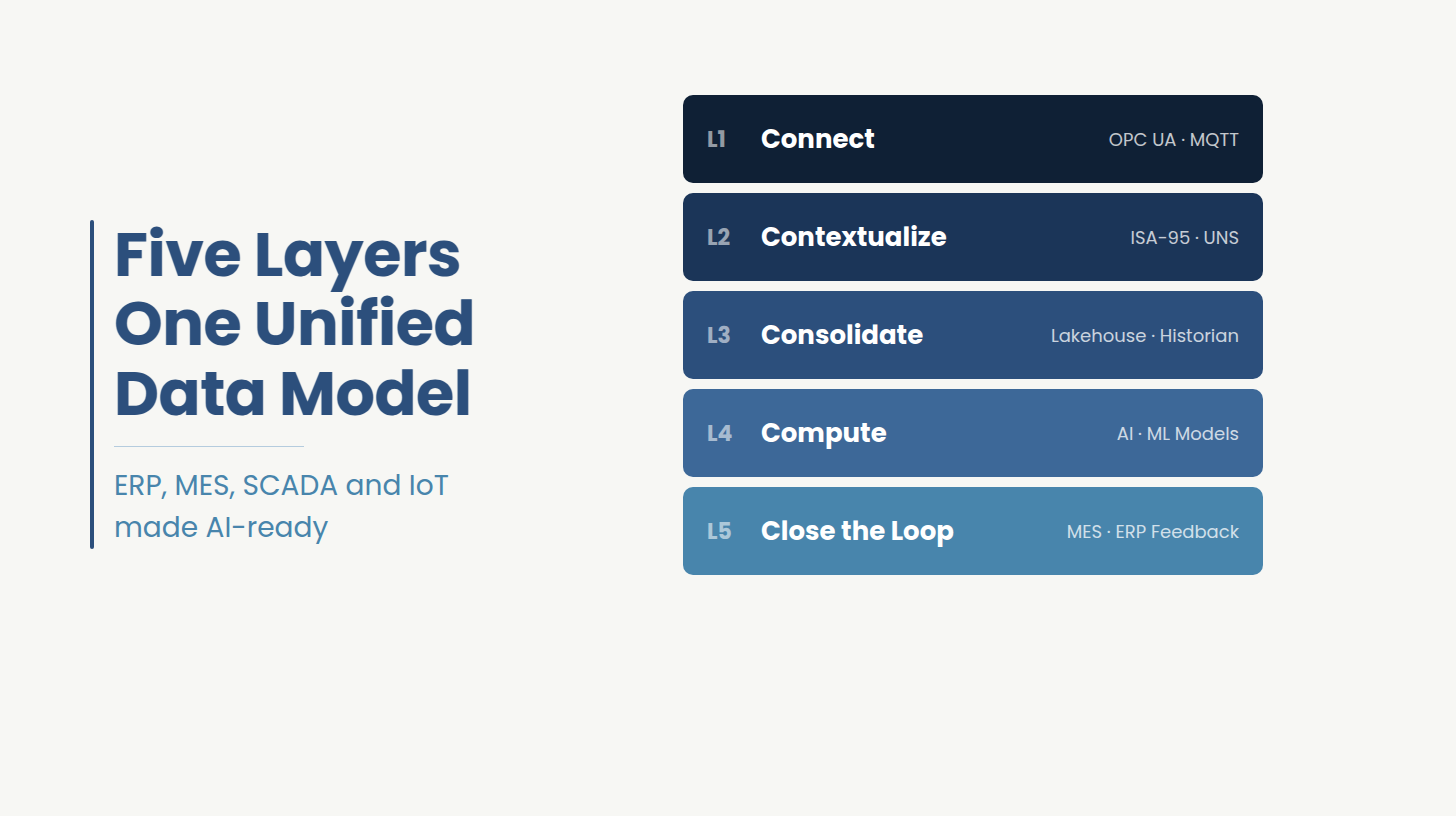
The right architecture for a custom medical imaging platform is not a single system. It is four distinct layers, each with a defined ownership boundary, and the boundary between what the health system controls and what a vendor can provide runs through the middle of the stack.
The foundation is the imaging data layer: DICOM-compliant storage, modality feeds from CT, MRI, ultrasound, and PET scanners, and the archive is whether a vendor-neutral archive or a custom object store. This layer can be vendor-provided without creating a Roadmap Ceiling problem, provided the data it holds is accessible in standard formats without vendor mediation. The moment imaging data is stored in a proprietary format that requires a vendor tool to read or export, the foundation carries a lock-in condition built into it from day one.
Above the data layer sits the AI orchestration layer. This is where model selection, inference routing, output formatting, and result delivery to the clinical workflow are managed. This layer must be owned by the health system. When the AI orchestration layer is embedded inside a vendor's PACS architecture, the health system cannot add, swap, or retire an AI model without vendor involvement. When the orchestration layer is owned and operated independently, model selection becomes an engineering and clinical decision. The difference between these two configurations is the difference between a health system that can act on a better lung nodule detection model the week it becomes available and one that must file a roadmap request.
The third layer is the EHR and RIS integration layer, built on HL7 FHIR for external interoperability and HL7 v2 for the internal hospital messaging that still carries most transactional workflow across large U.S. health systems. The 21st Century Cures Act and CMS interoperability rules require FHIR-based API access to patient health information legacy HL7 v2 feeds alone no longer satisfy federal interoperability mandates. Building EHR integration into a custom imaging platform from the architecture phase, rather than retrofitting it after the system is live, eliminates the middleware layer that costs health systems hundreds of thousands of dollars to build, own, and maintain across a contract lifecycle.
The fourth layer is the compliance boundary: HIPAA controls, PHI access governance, audit logging, encryption at rest and in transit, and the software lifecycle documentation required under IEC 62304 and the QMSR. This layer is not a feature added at the end of development. It is an architectural constraint that shapes every decision in the three layers below it. A platform built with the compliance boundary as a design input produces audit trails, access controls, and documentation artifacts as natural outputs of the development process. A platform that retrofits compliance after the build produces the same artifacts at materially higher cost and with greater regulatory exposure.
Medical imaging software is subject to six overlapping regulatory frameworks: HIPAA for patient data privacy and security; DICOM as the baseline standard for imaging data exchange and interoperability; HL7/FHIR as the federally mandated API standard for health information exchange under the 21st Century Cures Act; IEC 62304 for software lifecycle processes in medical device software; ISO 13485 for quality management systems across the device software development lifecycle; and FDA SaMD classification with 510(k) clearance for any software that makes or supports clinical decisions using AI. A custom imaging platform that handles all six from the architecture phase avoids the retrofit cost and the regulatory exposure of addressing them sequentially after the build.
The most consequential recent development is the enforcement of the FDA's Quality Management System Regulation on February 2, 2026. The QMSR formally aligns the FDA's existing Quality System Regulation with ISO 13485, meaning that any medical device software team that has historically operated under the FDA's QSR framework must now demonstrate ISO 13485-compatible quality management processes [8]. For health systems and development teams building AI-integrated imaging software, this is not a distant requirement. It is in effect now, and it applies to the development process itself. Teams that have been building AI diagnostics software without ISO 13485-aligned quality management documentation have a compliance gap that cannot be closed retroactively without a formal remediation program.
The FDA's January 2025 draft guidance on AI-enabled device software functions introduced a Total Product Lifecycle approach to AI medical device submissions [7]. The guidance recommends that marketing submissions include model descriptions, data lineage documentation, performance metrics tied to specific clinical claims, bias analysis and mitigation evidence, human-AI workflow descriptions, and post-market monitoring plans. In 2025, the FDA cleared 295 AI and ML-enabled medical devices, with 97% clearing via the 510(k) pathway at a median review time of 142 days [4] [5]. Radiology accounted for approximately 71.5% of those clearances [6]. The volume confirms that the pathway is navigable but the guidance raises the documentation bar for every submission that follows it.
HIPAA compliance in an AI-integrated imaging environment goes beyond encryption and access controls. When AI models process protected health information to generate diagnostic outputs, the PHI governance framework must cover the model inference pipeline itself . HIPAA-compliant development built into the AI orchestration layer from the architecture phase means audit logs, access controls, and minimum necessary use policies that apply to the model pipeline, not just the storage layer. A platform that treats HIPAA as a storage problem and leaves the inference pipeline ungoverned has a compliance gap that a HIPAA audit will find.
The practical implication of the 2025 and 2026 regulatory changes is that the compliance layer is becoming more demanding, not less. A health system evaluating a custom build or a PACS modernization today is evaluating it against a higher compliance baseline than existed two years ago. Vendors and development partners who cannot demonstrate QMSR-aligned quality management processes, AI lifecycle documentation practices, and HIPAA-governed inference pipeline architecture are not meeting the current standard. The compliance requirements described in this section apply equally to the evaluation of any development partner.
Custom medical imaging software development cost varies by scope, AI integration depth, regulatory classification requirements, and EHR integration complexity. The ranges below represent industry benchmarking figures synthesized across multiple development cost analyses they are planning anchors, not fixed quotes, and the factors that push scope from one tier to the next are described after the table.
Four factors push scope from the mid-market tier into the enterprise range with regularity. FDA SaMD classification required when the AI component makes or supports clinical decisions introduces a submission preparation burden that requires dedicated regulatory engineering time, bias analysis, and post-market monitoring design before a single line of production code ships. ISO 13485 and QMSR alignment, now enforceable as of February 2, 2026, requires quality management system documentation that must be built into the development process itself, not assembled after the fact. Multi-modality support compounds integration work non-linearly each additional imaging modality introduces its own DICOM profile, its own data volume characteristics, and its own AI model requirements. Data residency and security architecture increasingly required by state-level regulations and payer contracts adds infrastructure design work that is invisible in a basic scope but material in an enterprise one.
The break-even comparison with vendor-based alternatives requires honest framing. A custom build carries a higher upfront investment and a bounded total cost. A PACS vendor relationship carries a lower upfront cost and an unbounded total that compounds with every contract renewal, every storage upgrade, every per-study fee increase, and every middleware layer required to connect the imaging stack to clinical programs the vendor did not anticipate. Piedmont Healthcare realized more than $700,000 in savings after migrating away from a proprietary PACS model, with $2 million more projected as additional systems transitioned [9]. That figure represents the compounding vendor cost made visible once the exit is complete. A health system that builds custom on a five-year planning horizon is making a bounded investment against an unbounded recurring cost. The crossover point depends on volume, vendor contract terms, and AI program ambition, but for health systems in the enterprise tier with active AI diagnostics programs, most cost analyses place it between 18 and 36 months from deployment.
As a reference point: a health system processing 500,000 studies annually at a $2.50 per-study fee is paying $1.25 million per year to its PACS vendor. A custom platform in the $500,000 to $750,000 range reaches cost parity within 8 to 12 months on that volume alone, before any AI program revenue is factored in.
The vendor evaluation criteria that matter in medical imaging software development are not the ones that appear in RFP templates. They are the ones that map to the failure modes described in this guide integration architecture lock-in, undocumented legacy code, compliance gaps, and AI pipeline ownership. These six questions surface those failure modes before a contract is signed.
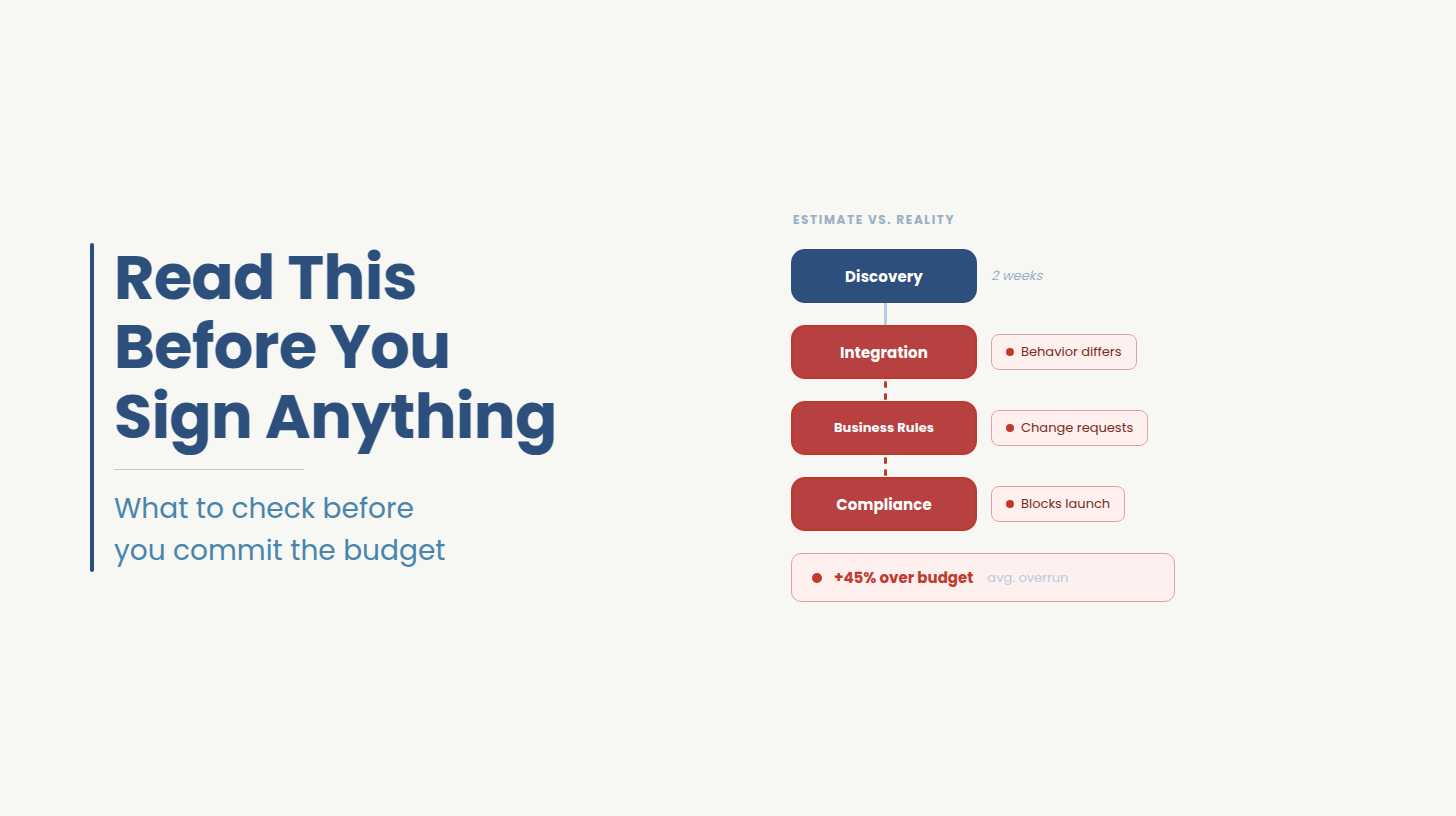
A strong answer describes specific technical onboarding on how the team connects to the existing DICOM stack, how they access the current EHR integration layer, and what they produce in the first two weeks. A weak answer describes a discovery phase that produces a requirements document before any engineering contact with the existing environment. Discovery phases that precede environment access consistently miss the undocumented dependencies that determine actual build complexity.
A strong answer names the classification pathway used, the submission documentation produced, and the IEC 62304 software lifecycle artifacts the engagement generated as standard outputs. A weak answer describes compliance as a final-phase activity or references a compliance consultant the partner brings in at the end. Compliance built into the development process produces documentation continuously. Compliance bolted on at the end produces a documentation sprint that regulators can identify.
A strong answer describes an architecture in which the health system owns the model registry, the inference routing configuration, and the output delivery pipeline and can modify any of them without involving the development partner. A weak answer describes an orchestration layer that runs on the partner's infrastructure or requires the partner's tooling to operate. An AI orchestration layer the health system cannot operate independently is a vendor dependency with a different name.
A strong answer describes a specific process for ingesting undocumented code like dependency mapping, automated analysis, documentation generation, and test coverage establishment before any modification begins. A weak answer describes a code review process that relies on developer judgment and tribal knowledge. Undocumented legacy PACS code that is modified without a prior documentation and analysis phase introduces regression risk that compounds with every subsequent change.
A strong answer names a specific artifact like a dependency map, an AI readiness analysis, a modernization blueprint, a scoped architecture recommendation and confirms the health system owns it regardless of whether the engagement continues. A weak answer describes a relationship-building period or a planning phase with no defined output. The first-month deliverable is the clearest signal of how the rest of the engagement will be structured. Partners who cannot name it have not structured the engagement around the health system's decision-making needs.
A strong answer specifies that the health system receives full ownership of all production code, all documentation artifacts, all test coverage, and all compliance documentation in standard formats the health system can operate, modify, and hand to a different partner without restriction. A weak answer introduces licensing terms, platform dependencies, or ongoing support requirements that create a new form of the vendor dependency the health system was trying to exit. Codebase ownership language in a development contract deserves the same scrutiny as integration architecture language in a PACS contract.
Ideas2IT's healthcare engineering team holds AWS Healthcare Competency, is SOC 2 Type II certified, and operates HIPAA-compliant delivery infrastructure. Engineers embed inside the client's existing DICOM and EHR environment from day one rather than working from a requirements document. The entry point is a no-cost imaging stack assessment that maps the current PACS dependency structure and delivers a written recommendation with cost and timeline ranges across three paths: modernize, replace, or build custom. To start the assessment, visit Ideas2IT's custom software development practice.
[1] Mordor Intelligence. "Medical Imaging Software Market." Mordor Intelligence Industry Reports. 2025. https://www.mordorintelligence.com/industry-reports/medical-imaging-software-market-industry
[2] Mechanical Orchard. "$1.14 Trillion to Keep the Lights On: Legacy's Drag on Productivity." Mechanical Orchard Insights. 2024. https://www.mechanical-orchard.com/insights/1-14-trillion-to-keep-the-lights-on-legacys-drag-on-productivity
[3] HIMSS Analytics. "Healthcare IT Legacy Systems Study." HIMSS Analytics. 2024. Cited in: World Wide Technology. https://www.wwt.com/blog/the-hidden-cost-of-legacy-systems-building-the-business-case-for-healthcare-it-modernization
[4] Innolitics. "2025 Year in Review: AI/ML Medical Device 510(k) Clearances." December 2025. https://innolitics.com/articles/year-in-review-ai-ml-medical-device-k-clearances/
[5] ICON plc. "Understanding FDA Regulations for AI in SaMD." June 2025. https://www.iconplc.com/insights/blog/2025/06/24/fda-regulations-ai-medical-devices
[6] IntuitionLabs. "FDA Pathways for AI SaMD: 510(k), De Novo and PMA Guide." April 2026. https://intuitionlabs.ai/articles/fda-samd-pathways-510k-de-novo-pma-ai
[7] U.S. Food and Drug Administration. "AI-Enabled Device Software Functions: Lifecycle Management Recommendations (Draft Guidance)." January 6, 2025. https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-software-medical-device
[8] IntuitionLabs. "FDA SaMD Classification: AI and Machine Learning Guide." April 2026. https://intuitionlabs.ai/articles/fda-samd-classification-ai-machine-learning
[9] Hyland. "Overcoming the PACS Software Cost Conundrum." Hyland Healthcare. https://www.hyland.com/en/resources/articles/overcoming-the-pacs-cost-conundrum
[10] Hyland. "Overcoming the PACS Software Cost Conundrum." Hyland Healthcare. https://www.hyland.com/en/resources/articles/overcoming-the-pacs-cost-conundrum