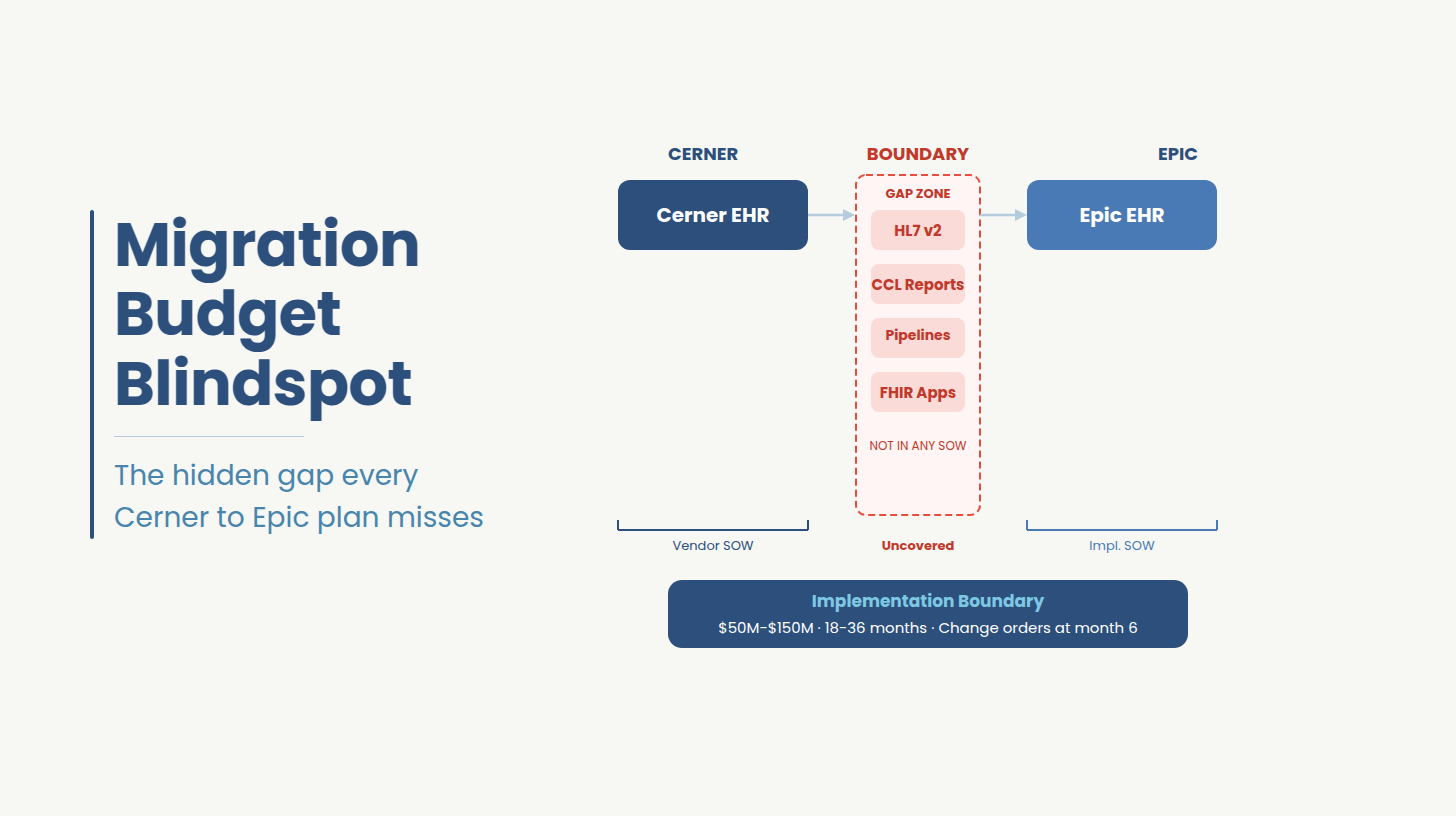
Most custom FHIR integration hub projects for hospitals never reach production because the two most expensive variables in the project were excluded from the first quote: bidirectional write-back complexity and the EHR certification path. By the time both surface, the budget has been approved, the SOW has been signed, and the change orders have already begun.
The first vendor quote you received for your FHIR integration project was probably $40,000-$60,000. The actual cost, if the project reaches production, will likely be two to three times that. The gap is a scoping granularity problem that repeats across every hospital FHIR engagement.
The administrative burden this gap creates is not abstract. According to the AMA's prior authorization survey[4], physicians complete an average of 39 prior authorization requests per week and spend 13 hours processing them, time that a functioning FHIR-based automation layer is specifically designed to reclaim. When integration projects overrun on cost and timeline, hospitals defer that automation, and the clinical and administrative costs compound.
This piece addresses the hospital IT leader who has already decided to build a custom FHIR integration hub and needs to make four decisions correctly: which architecture pattern to commit to, what the realistic cost and timeline look like, which delivery model fits the organization's risk tolerance, and who should own technical accountability throughout execution. Those four decisions, made with accurate information, determine whether the project ships to production or joins the archive of delayed initiatives.
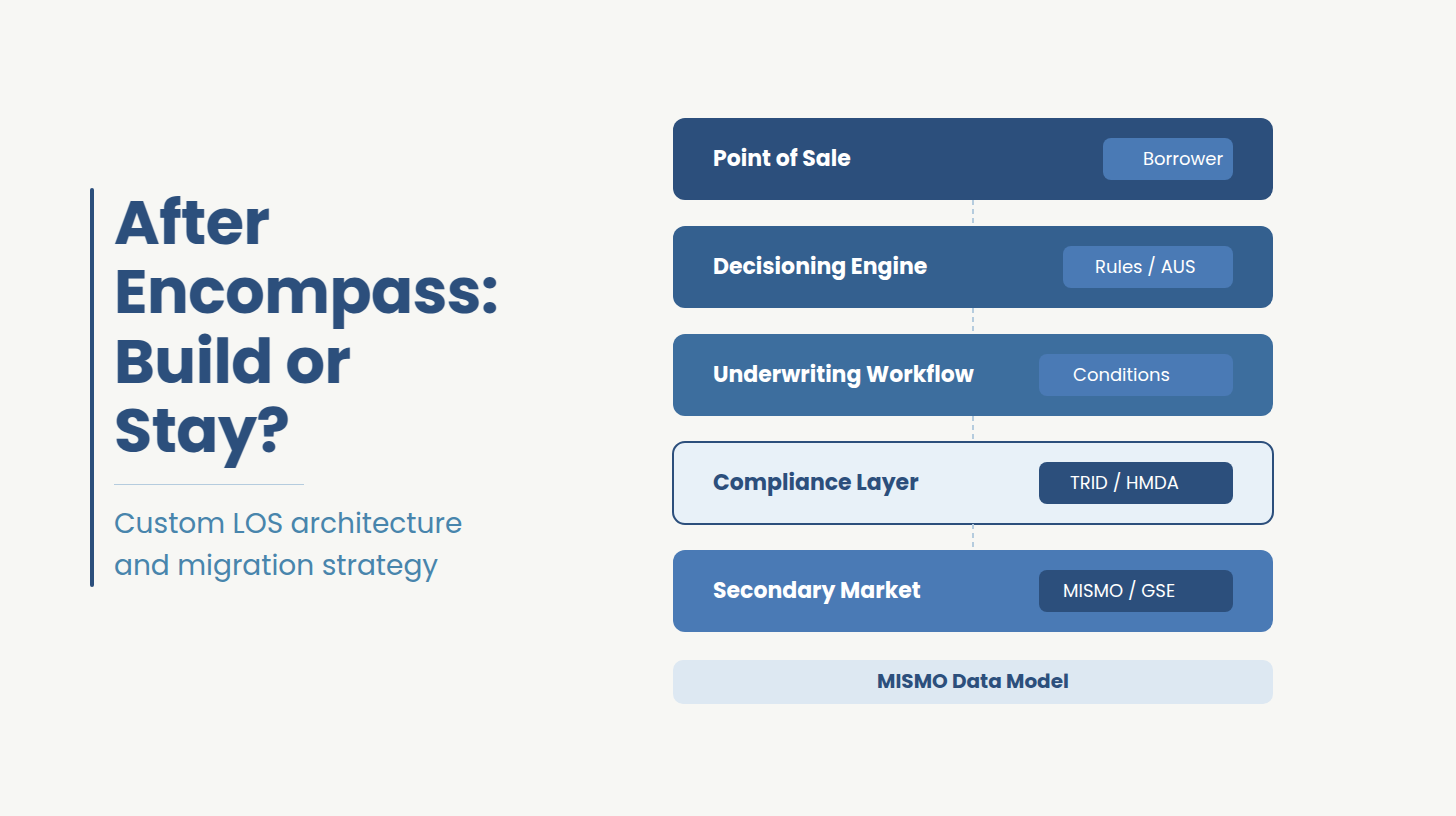
Every hospital FHIR integration hub is built on one of two patterns, and the choice is largely irreversible once data flows begin in production. The pattern you select in the first four weeks of a project will constrain every architectural decision that follows.
A FHIR facade sits in front of existing EHR systems and translates API queries in real time. Source data stays in the originating system and the hub is a translation layer. This pattern is faster to stand up and operationally lower risk because there is no data synchronization problem to manage. Its ceiling is also lower: real-time query performance degrades at scale, and cross-EHR analytics require federation logic or a downstream data pull regardless.
A FHIR repository ingests, normalizes, and stores FHIR R4 resources. The hub becomes a parallel system of record for defined data domains. This pattern supports richer analytics, population health pipelines, and clinical AI workloads but introduces data governance obligations, synchronization lag, and ongoing maintenance of a data asset that the organization now owns. For health systems running multiple EHRs or planning AI/ML workloads within two years, a repository pattern is typically the sound long-term call.
Most hospitals that have built a FHIR layer started with a facade and called it done. When they later need write-back workflows or analytics at scale, they discover that retrofitting repository semantics onto a facade architecture needs a complete rebuild.
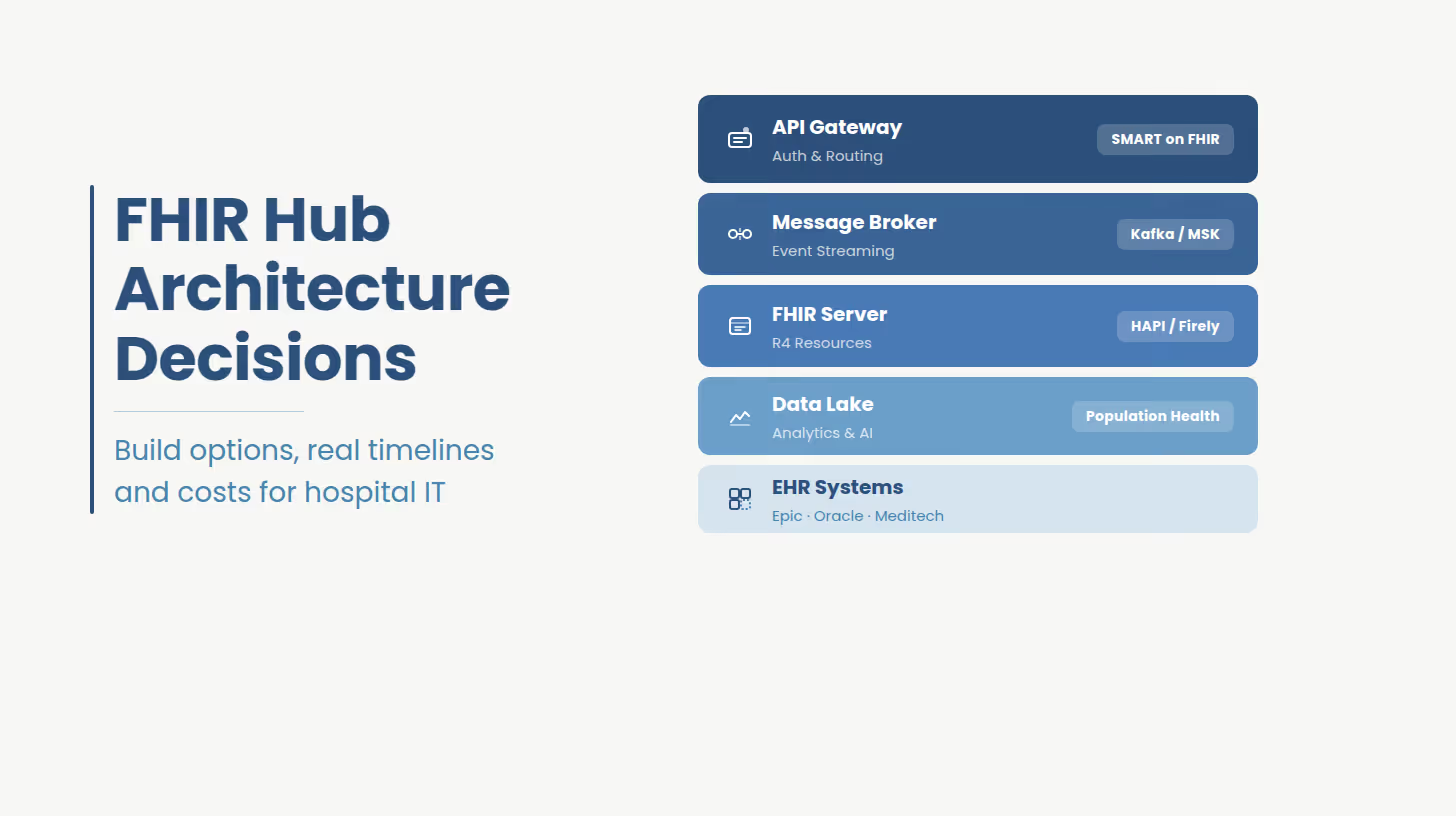
A production-grade FHIR integration hub has four layers: an API gateway handling authentication, rate limiting, and routing; a message broker (Apache Kafka or AWS MSK at scale, RabbitMQ for simpler deployments) managing asynchronous event streams; a FHIR server storing and serving normalized R4 resources; and a data lake or warehouse layer for analytics workloads. HIPAA-compliant audit logging, SMART on FHIR OAuth 2.0 authorization flows, and US Core Implementation Guide validation run across all four layers.
FHIR server selection is where projects routinely stall. HAPI FHIR is open-source, community-supported, and the default for organizations that want maximum control at zero licensing cost but it requires engineering investment to production-harden. Firely Server is commercially supported, R4 and R5 compliant, and easier to certify for enterprise deployments, but carries licensing cost. AWS HealthLake and Google Cloud Healthcare API are managed services that compress deployment time but introduce cloud dependency and data residency questions that compliance teams will surface. The right answer depends on existing cloud posture, internal engineering bandwidth, and the organization's build-and-own appetite relative to managed support cost.
The FHIR version question also deserves a direct answer. FHIR R4 remains the standard for US regulatory compliance and is the primary version used by 22 of 38 respondents in the 2024 State of FHIR Survey.[5] Epic's production Interconnect API runs R4. Designs targeting R5 for net-new enterprise hubs are emerging, but R4 is the safe compliance baseline for any project with a 2026 go-live requirement.
Is your FHIR architecture decision reversible?
If you are mid-scoping or have received a first vendor quote, a 90-minute architecture review with Ideas2IT's FHIR engineering team will surface write-back complexity, certification dependencies, and delivery model tradeoffs before they become change orders.
Request a FHIR Architecture Review
A read-only single-EHR FHIR integration takes 8 to 14 weeks when Epic App Orchard certification is included. Bidirectional write-back to a production Epic environment takes 18 to 30 weeks. A multi-EHR enterprise hub runs 12 to 18 months. Epic's certification queue, not the build itself, is the variable that most consistently breaks hospital project timelines.
The phase breakdown that matters for budget and governance planning runs five stages:
Epic's App Orchard certification is the timeline variable that surprises health systems most consistently. Epic's review queue operates on Epic's schedule, not the project's. Certification reviews take four to eight weeks after submission, and submissions frequently require multiple revision rounds. Projects that do not begin the certification application in parallel with the build phase regularly extend by months on this dependency alone.
The HL7 v2 to FHIR transformation layer is the second major timeline risk. Most legacy hospital systems still emit HL7 v2 messages. Transformation logic for complex message types particularly MDM (medical document management) and complex ORM/ORU workflows is hospital-specific and requires mapping documentation that often does not exist, meaning engineering time to reverse-engineer it from live system behavior.
The knowledge gap is structural. The 2024 State of FHIR Survey found that lack of FHIR expertise was cited as the biggest barrier to adoption for the second consecutive year by more than three-quarters of respondents.[3] Organizations that treat FHIR expertise as a commodity hire routinely discover the gap mid-project.
Cost ranges for FHIR integration projects are wide because the scope variables are large. A read-only interface between two systems with documented data models costs substantially less than a bidirectional write-back layer to a production Epic environment that has been customized over fifteen years of local configuration. Both are FHIR integrations. Their costs have nothing to do with each other.
Healthcare organizations implementing FHIR-based interoperability report a return of $3.20 for every $1 invested[6] but that ROI only materializes when the implementation reaches production and operates correctly. Projects that overrun on cost or timeline due to scoping errors produce the opposite outcome.
"Epic and Oracle Health both charge for API access configuration. Epic's Interconnect licensing is a recurring annual cost. Industry benchmarks place EHR interoperability API fees at $1,000 to $10,000 per integration per year. These fees do not appear in implementation quotes from development partners because they are billed directly by the EHR vendor, not the integrator.
For a hospital running five integrations against a production Epic environment, this is $5,000 to $50,000 in annual recurring cost that the initial budget conversation never surfaces. On a five-year TCO basis, this line item alone can shift the build vs buy calculation.
The build vs. buy decision for a FHIR integration hub is not primarily a cost decision. It is a control and roadmap decision. The cost differential between a custom build and a managed platform compresses significantly when platform subscription costs are annualized over three years against a custom build with no recurring per-connection fee. The more decisive questions are about data ownership, customization ceiling, and what happens when the platform vendor's roadmap diverges from the hospital's clinical workflow requirements.
The market is moving toward interoperability investment at a structural level: according to Gartner, 62% of US health systems now classify interoperability as a 'critical strategic investment,' compared to 23% in 2023, with average interoperability spending increasing to 18% of total IT budgets.[8]
Custom build is the right call when three conditions hold: the hospital has clinical workflows no commercial platform supports out of the box; the organization has or is building an AI/ML roadmap that requires direct FHIR data access without per-query fees; and the hospital has either internal engineering capacity or a delivery partner who can own the FHIR engineering function long-term. Academic medical centers with research data requirements, health systems running five or more EHRs, and organizations with population health platforms that need real-time FHIR write-back consistently meet these conditions.
Platform-first is the sound choice when the hospital has a single EHR, a defined interoperability use case (payer connectivity, prior authorization), and no internal FHIR engineering capacity. In this scenario, three years of platform SaaS cost is typically lower than the organizational cost of owning a custom hub with no internal engineering succession plan.
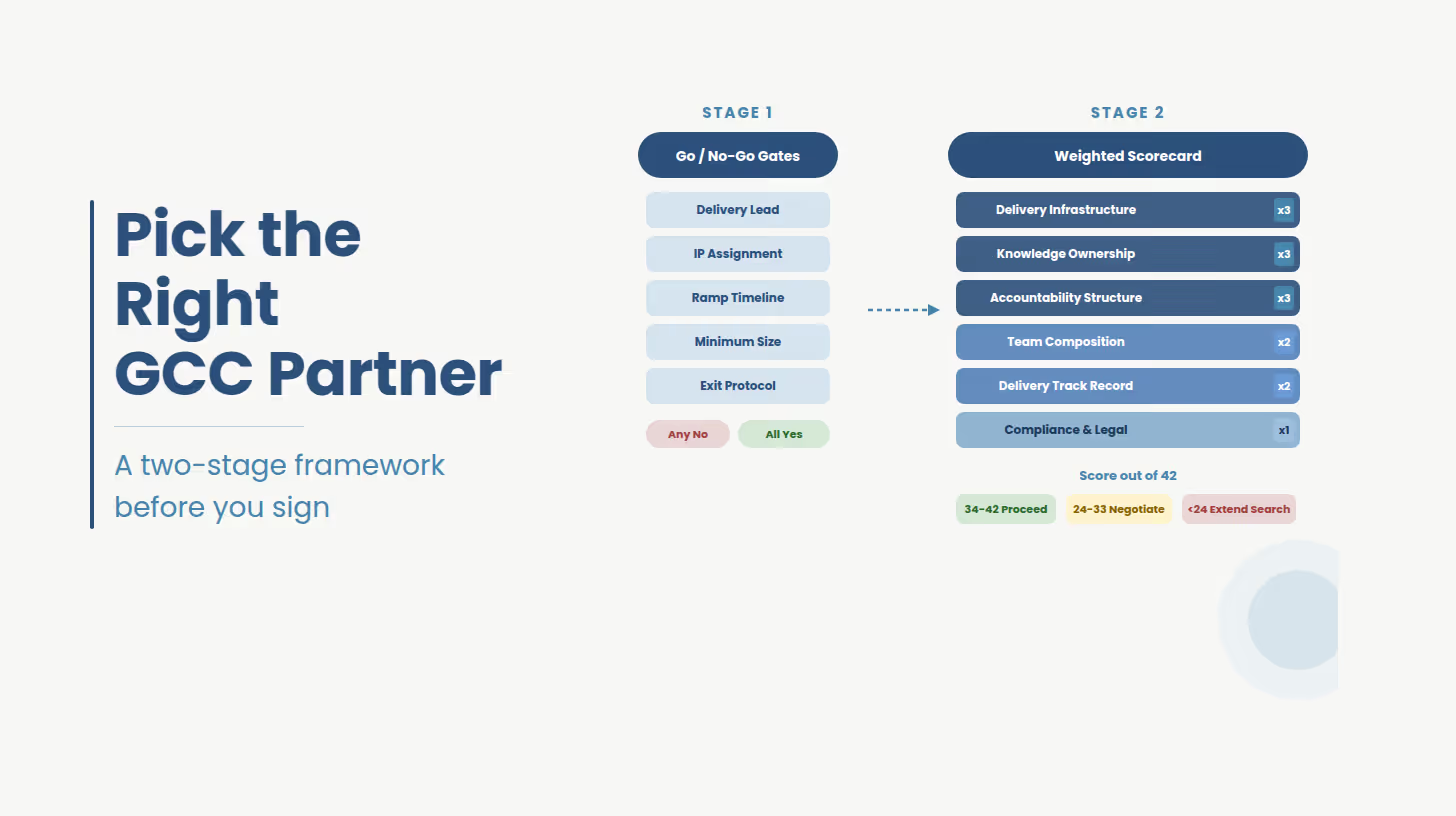
The most consequential and least-discussed variable in a FHIR integration project is the delivery model about how accountability is structured throughout delivery and into production operations. Four models exist in this market. Each produces a different risk profile.
Fixed-scope delivery works when integration requirements are fully documented, the EHR vendor's API behavior in the hospital's specific configuration is well-understood, and both parties have enough shared FHIR expertise to define done precisely.
The risk: FHIR integration scopes are rarely stable once discovery begins. Hidden EHR customizations surface during build, and fixed-scope contracts generate change orders rather than conversations.
Time-and-materials delivery transfers scope risk to the hospital. It is appropriate when requirements are genuinely exploratory, a first-generation FHIR hub where architecture is being validated through build.
The risk: without a delivery partner who proactively surfaces scope and timeline decisions rather than executing against hours, T&M projects drift.
Managed service delivery is the model most underserved hospital IT organizations need and most vendors do not offer for FHIR. The delivery partner owns the engineering, operations, and compliance posture of the hub as a service. The hospital retains architectural governance but does not need to staff FHIR engineering internally. For organizations without a succession plan for the FHIR expertise the project requires, this model eliminates the most common reason FHIR projects succeed in build and fail in production.
Staff augmentation embedding FHIR-specialized engineers into the hospital's IT organization is appropriate when the hospital has architectural ownership capacity but lacks specific FHIR, HL7, or SMART on FHIR depth. It is the most flexible model and the most susceptible to delivery quality variance: FHIR engineering skill distribution across the contractor market is uneven, and the knowledge gap is structural.[3]
The CMS-0057-F Interoperability and Prior Authorization rule has entered its phased compliance period. Operational requirements including the 72-hour decision timeframe for urgent prior authorization requests and the 7-day standard for routine requests took effect January 1, 2026.[2] The FHIR Prior Authorization API requirements move to a January 1, 2027 go-live deadline.
The downstream implication for hospitals: any organization that exchanges prior authorization data with affected payers (Medicare Advantage, Medicaid managed care, ACA marketplace plans) and has not begun FHIR API integration planning is inside the critical path for the 2027 deadline. With Epic App Orchard certification adding four to eight weeks to delivery timelines, and bidirectional integration builds running 10-18 weeks before certification is submitted, a 2027 go-live requires project kickoff no later than Q2 2026 a window that is closing now.
The scale of the problem this mandate is designed to address: physicians currently complete an average of 39 prior authorization requests per week, spending 13 hours on the process[4], and 93% of surveyed physicians report that prior authorization delays patient care. The CMS mandate creates a compliance forcing function, but the hospital-side FHIR infrastructure to connect with payer APIs is the hospital's responsibility to build and maintain.
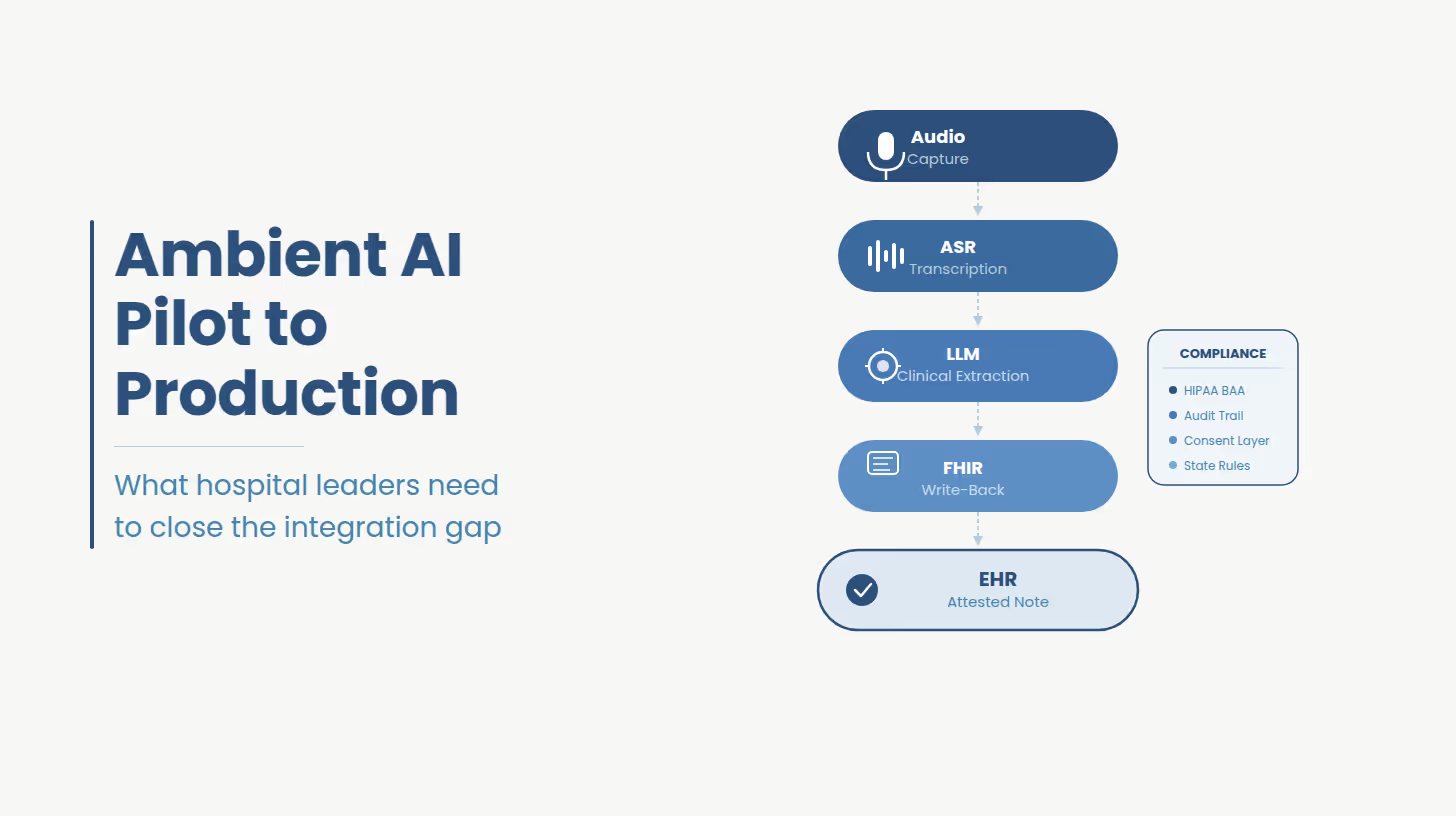
HIPAA compliance instrumentation for FHIR is more involved than standard HIPAA BAA paperwork. The combination of SMART on FHIR OAuth 2.0 authorization flows, FHIR AuditEvent resources, and US Core IG consent and provenance requirements creates a compliance surface that requires dedicated security architecture work. Organizations that treat it as documentation rather than an engineering design requirement typically discover the gap during EHR vendor certification reviews which is the worst possible time to surface it.
The regulatory direction is clear: 73% of countries surveyed in the 2025 State of FHIR report now either mandate or recommend FHIR usage, up from 65% in 2024 and 56% in 2023.[9] For US hospitals, the mandate is timestamped.
What the January 1, 2027 requirement specifically means for hospitals: any organization exchanging prior authorization data with Medicare Advantage plans, Medicaid managed care organizations, or ACA marketplace payers must expose a FHIR Prior Authorization API that meets the HL7 Da Vinci implementation guide specifications. The hospital-side infrastructure to connect with those payer APIs is the hospital's responsibility to build, certify, and maintain. Payer readiness does not substitute for hospital readiness.
Every architectural decision in this piece facade vs. repository, HAPI vs. Firely, fixed scope vs. managed service is technically revisable in theory. In practice, the decisions made in the first six weeks of a FHIR integration project calcify into production constraints that persist for years. The delivery partner who owns those first six weeks determines the quality of every constraint that follows.
Ideas2IT has been building healthcare data integration systems since 2017. Our FHIR engineering practice includes specialists in Epic Interconnect, Oracle Health SMART on FHIR, HL7 v2 to FHIR transformation pipelines, and HIPAA-compliant API architecture. We deploy Forward Deployed Engineers instead of contractors and project managers who embed in the hospital's existing IT environment from Day 0, working inside the same ticketing systems, standups, and architecture review cadences as internal teams.
For FHIR integration projects, our delivery is backed by Legacyleap, our agentic modernization platform that replaces six to eight weeks of manual discovery with one week of automated codebase and interface analysis. On a FHIR integration project, this compresses the architecture validation phase where most projects lose the most time and where write-back complexity and EHR certification dependencies are surfaced or missed.
A regional health system integrating a population health analytics platform with Epic and Meditech across twelve hospitals engaged Ideas2IT for a hub-and-spoke FHIR repository build. Legacyleap's automated discovery surfaced four undocumented Epic customizations in the medication administration record that would have become production defects post-certification. The project went live two months ahead of the original estimate with zero post-launch rollback events.
Our healthcare engineering team holds AWS Healthcare Competency certification, SOC 2 Type II, and ISO 27001, and operates under HIPAA Business Associate Agreements as a standard delivery condition. The 99% client renewal rate across Ideas2IT's healthcare practice reflects what happens when FHIR expertise is matched to organizational accountability.
If you are in active scoping for a FHIR integration hub, the highest-value hour you can spend before the next vendor conversation is a structured architecture review that surfaces write-back complexity, the EHR certification path, and the delivery model fit for your organization's risk tolerance.
Ideas2IT offers a no-cost FHIR Integration Architecture Review: a 90-minute working session with senior FHIR engineering and a written summary of architecture options, realistic timeline ranges, and delivery model recommendations specific to your EHR environment and integration objectives. A technical working session designed to produce a decision frame you can take into your budget conversation.
Schedule your FHIR Architecture Review
Didn't find what you were looking for?