Four hours after go-live, a department head called the CTO. The population health dashboard managing chronic disease panels across 40,000 attributed lives was showing no data. The pipeline feeding it was built against Cerner's data model three years earlier. It was not in the implementation partner's SOW. It was not in Epic's migration scope. It stopped working the moment the Cerner environment went offline. This is the default outcome when a migration budgets for the EHR switch and ignores the decade of custom infrastructure sitting underneath it.
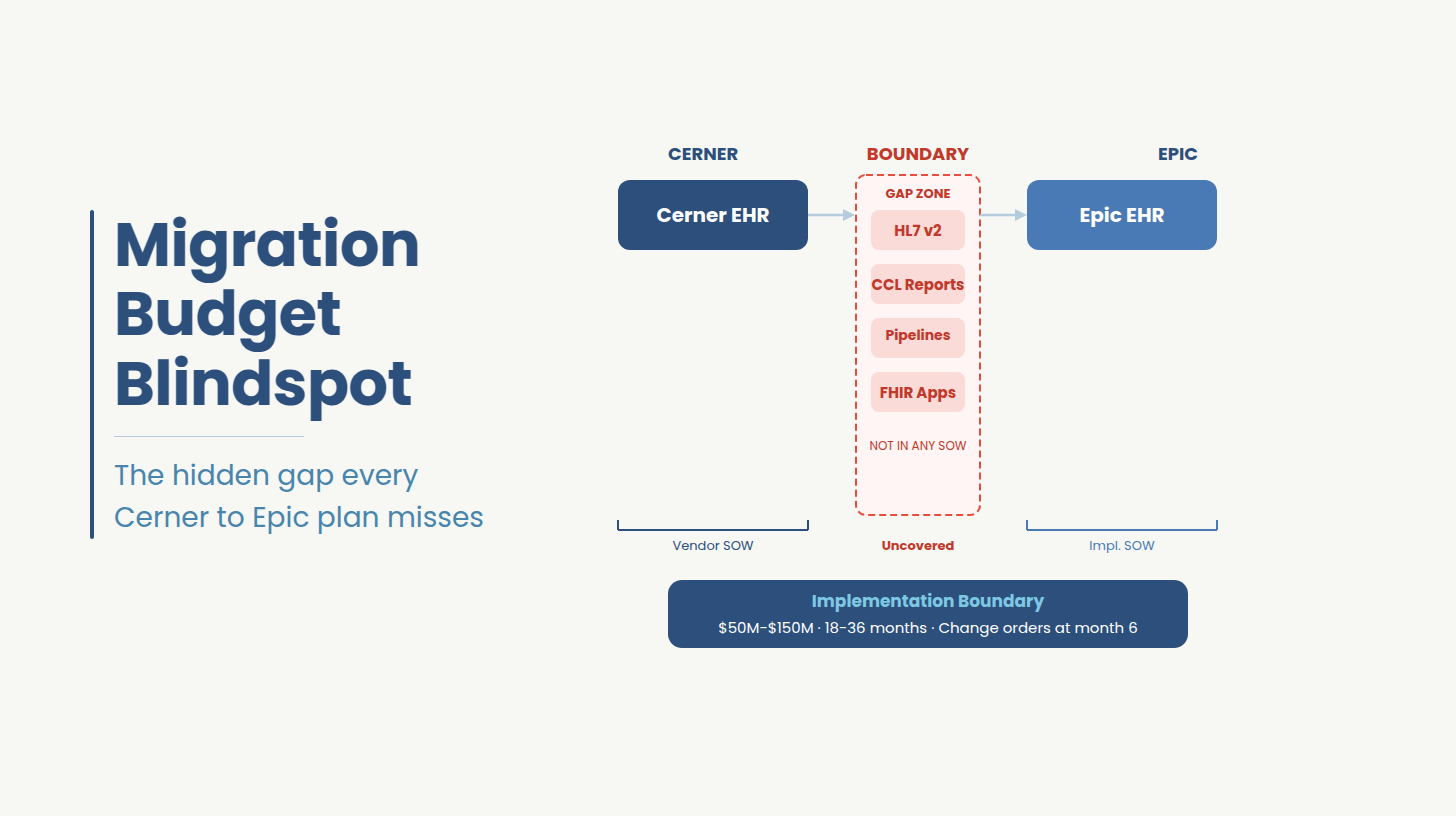
What they are looking at is the Implementation Boundary, the point at which the vendor's contract ends and the health system's custom-built data infrastructure begins.
The Implementation Boundary is the structural gap between the EHR vendor's contract scope and the health system's custom-built data infrastructure: the HL7 integrations, CCL reports, data pipelines, and FHIR applications that neither the vendor nor the implementation consultant owns.
This is a structural gap that exists in every Cerner-to-Epic migration because the EHR vendor's contract ends before the custom engineering layer begins, and the implementation consultant's SOW ends at the same place. The decade of HL7 integrations, CCL reports, data pipelines, and FHIR-facing applications built on Cerner's architecture sits in a gap that no contract covers and no migration timeline accounts for.
This article covers the layer that every migration plan misses and what it costs when it is not scoped before the program starts.
Oracle acquired Cerner for $28 billion in June 2022. The strategic logic was clear: a cloud infrastructure company absorbing the second-largest EHR vendor in the U.S. would produce an integrated clinical-and-cloud platform at a scale no competitor could match. What followed was something different.
Within 18 months of the acquisition, Oracle had reportedly reduced the Cerner workforce by approximately 50%. The immediate consequence was a support gap. Health systems that had escalation relationships with Cerner's implementation and engineering teams found those relationships severed. Roadmap commitments made before the acquisition became difficult to track. Customer advisory inputs that had shaped Cerner's development priorities stopped producing visible results.
The VA contract made the delivery problem visible at national scale. The Department of Veterans Affairs had awarded Cerner a contract ultimately valued at more than $16 billion to deploy a unified EHR across 170 VA hospitals. By the time the program was paused in 2023 following documented patient safety incidents, six of those hospitals were live. Congressional criticism was bipartisan. The program became the most public evidence that Oracle Health's delivery capacity did not match its contract commitments and health system CIOs who had been watching drew their own conclusions.
The third forcing function was quieter but operationally significant. Cerner built its developer API layer, Cerner Ignite on FHIR DSTU2, a standard that predates the current FHIR R4 mandate. Oracle Health has announced the deprecation of DSTU2, which creates a forced modernization obligation for every health system and ISV running applications against Cerner's API layer. That obligation exists on its own timeline, independent of the EHR migration decision. For health systems already committed to Epic, it compresses the window further. For those still on Cerner, it is a separate program that now competes for the same internal engineering capacity.
Taken together, these three developments did not simply validate Epic as the destination. They started the clock on migration programs that many health systems had not fully scoped and that clock is not pausing while the scoping catches up.
Epic now holds approximately 42% of U.S. acute care beds. That number matters less as a market share statistic and more as a network effect: when a health system's referral partners, payer contracts, and regional IDN affiliates are all running Epic's Care Everywhere interoperability layer, the decision to join that network is not purely a product evaluation. It is an infrastructure alignment decision with compounding consequences over time.
The physician satisfaction data accelerated what the network effect started. When Intermountain Health conducted an internal evaluation across its physician and APP population, 98.5% consensus emerged for Epic based on functional capability and satisfaction scores. That figure is unusual in healthcare IT, where clinical staff resistance is the most consistently underestimated implementation risk. A health system that can point to that level of clinician alignment has removed the single variable most likely to cause a migration to fail on the operational side.
The permanence is the point. A health system that has aligned its referral network, payer contracts, clinical staff, and capital program to Epic's architecture has closed a door behind it. That irreversibility is what makes the Implementation Boundary consequential. The second project inside it has to get done regardless of how hard it is, how late it surfaces, or how unprepared the program budget is to absorb it.
While Oracle Health's delivery capacity contracted, Epic's network reached a scale that made the migration decision self-reinforcing. When referral partners, payer contracts, and regional affiliates all run Care Everywhere, joining that network is an infrastructure alignment decision, not a product evaluation.
Cerner Millennium's interface engine processes custom HL7 v2 messages through configuration that is native to Cerner's data model: trigger events, segment structures, field-level mappings, and acknowledgment logic built specifically for Cerner's architecture. Epic Bridges does not import that configuration. Every interface must be rebuilt from the message level: the trigger event, the segment structure, the field mapping to Epic's data model, and the acknowledgment behavior. For a mid-sized IDN, that is typically 150 to 250 individual rebuild projects, each requiring a full testing cycle against the receiving system before the cutover window. An interface that fails testing on go-live eve does not delay go-live. It goes live broken, and the connected system receives no data until the interface is fixed in production.
Most health systems enter a migration estimating 60 to 80 active CCL reports. A full extraction from the Cerner environment typically returns three to five times that number, because report-writing access in Cerner was distributed rather than governed. Reports built by analysts, department coordinators, and former employees who have since left are still running in production. No one knows who owns them, no one knows what decisions they support, and no one knows which ones will cause an operational failure if they stop on go-live day. That triage work alone consumes engineering weeks that no implementation timeline budgeted for.
The third is data pipelines. Clinical analytics platforms, population health tools, and revenue cycle dashboards that pull from Cerner's data model do not automatically repoint to Epic's. Epic's data model is structurally different from Cerner Millennium's. Pipelines built against Cerner's schema require re-engineering, not reconfiguration.
The fourth is SMART on FHIR applications. Applications certified against Cerner Ignite's DSTU2 API layer face deprecation regardless of whether the hospital migrates. This category of work sits inside the Implementation Boundary but operates on a separate timeline, which the following section addresses directly.
As one Trinity Health CIO documented mid-program: "Failure to prioritize data hygiene on the front end risks automating inconsistencies or migrating erroneous data — which ultimately compromises operations, revenue and patient care." The Implementation Boundary is where that front-end work lives. It is also where most programs discover, too late, that it was never assigned to anyone.
Cerner built its developer API layer, Cerner Ignite on FHIR DSTU2, a specification that predates the current federal interoperability mandate by several years. Oracle Health has announced the deprecation of DSTU2, which means every SMART on FHIR application running against Cerner Ignite must be re-certified against FHIR R4. This is known as DSTU2 deprecation. It exists on its own deadline, issued by Oracle Health, independent of any decision the health system makes about its EHR.
For health systems already committed to Epic, DSTU2 deprecation creates a sequencing problem. The internal IT team managing SMART app re-certification is competing for the same integration testing windows, clinical validation resources, and go-live engineering capacity as the Epic implementation program. Both programs need the same people and have hard deadlines. Neither program's vendor owns the conflict between them.
For healthcare ISVs who built on Cerner Ignite, the problem is more direct. An ISV whose application is certified against DSTU2 faces a re-engineering and re-certification requirement on a timeline set by Oracle while their primary hospital clients are simultaneously managing Epic go-lives. The ISV cannot control the hospital's go-live schedule. The hospital cannot control the Oracle deprecation deadline. The conflict lands in the ISV's engineering roadmap as an unplanned priority that competes with every other development commitment already in flight.
The business consequence is specific: application downtime at the worst possible moment, re-certification cost that was not in the product budget, and the risk that a hospital go-live surfaces a broken third-party application in the first week of Epic operations when clinical staff tolerance for system failures is at its lowest and IT credibility is at its most exposed.
DSTU2 deprecation is not a migration sub-task. It is a parallel compliance program that intersects with the migration timeline at multiple points and belongs in the Implementation Boundary inventory from day one.
For mid-to-large health systems, a Cerner-to-Epic migration typically runs $50 million to $150 million or more, with timelines of 18 to 36 months from program kickoff to go-live.
A change order for 200 HL7 interface rebuilds runs $1 million to $3 million depending on interface complexity and the implementation partner's rate structure. CCL report conversion at scale, when scoped mid-program after the full inventory surfaces, adds $500,000 to $1.5 million in unplanned engineering cost. These figures do not appear in the original implementation budget because they do not appear in any vendor's SOW. They appear six to twelve months into the program, when the go-live date is fixed, the internal team has no capacity, and the program has no budget flexibility left to absorb them.
Both figures assume a well-governed program with executive sponsorship, a seasoned implementation partner, and a clean data environment. In practice, all three of those assumptions fail at some point in every program.
The budget lines that are well-scoped Epic licensing, implementation partner fees, infrastructure, training rarely produce the surprises. The surprises come from the Implementation Boundary. Custom integration rebuilding, CCL report conversion, data pipeline re-engineering, and FHIR re-certification work surface as change orders at the worst possible moment: 6 to 12 months into the program, when the implementation partner is deep in build, the internal team is stretched across workstreams, and the go-live date has become a fixed political commitment.
The single most underestimated timeline risk sits earlier than most program managers expect. Database backups from Cerner Millennium required before any data extraction or migration work can begin can take up to six months to obtain. If backup retrieval is not initiated at program kickoff, it silently consumes the contingency buffer before the integration rebuilding workstream has started. A program that initiates backup retrieval at month three instead of month one does not recover those two months. It absorbs them as schedule compression later, when compression is most damaging.
The structural problem is that the Implementation Boundary does not appear as a named budget line in most program plans because it does not appear in any vendor's SOW. It is missing because neither the EHR vendor nor the implementation consultant has a contractual reason to put it there. It appears when something breaks: a change order, an emergency engagement, or a post-go-live remediation program that costs significantly more than scoping it upfront would have.
If your program has not inventoried the custom integrations, CCL reports, and data pipelines sitting on the Cerner side of your Implementation Boundary, that gap will surface as a change order or a go-live incident. Ideas2IT offers a no-cost scoping conversation to map what is there before it becomes a problem.
Schedule a conversation
Cerner Millennium database backups required for data extraction can take up to six months to obtain from Oracle Health. This is not a risk that careful project management prevents. It is a vendor-controlled process with a vendor-controlled timeline. A program that initiates backup retrieval at month three instead of month one does not recover those two months. They are absorbed as schedule compression in the final phases of the program, when the implementation team is at peak load, the go-live date is a political commitment, and compression causes the most damage. Backup retrieval initiation on day one of the program is not optional. It is the single timeline action with the longest lead time and the least flexibility.
The health systems that avoided post-go-live failures did not have larger budgets or more favorable timelines. They made one structural decision that most programs do not: they treated the Implementation Boundary as a parallel workstream with its own engineering ownership, its own timeline, and its own go/no-go criteria before the implementation contract was signed.
The first thing they did differently was inventory before they committed. Not a technical audit conducted during discovery, but a business-consequence mapping exercise conducted internally: every CCL report mapped to the business owner who depends on it, every custom HL7 interface mapped to the operational process it supports, every data pipeline mapped to the clinical or financial decision it informs. The output was a risk register that named what would break on go-live day if each item was not rebuilt in time and who in the organization would feel it.
The second was assigning engineering accountability independently of the implementation program. The Implementation Boundary requires a separate engineering team with a separate scope, a separate timeline, and direct accountability to the health system's go-live date. Health systems that conflated these two workstreams consistently found that the implementation partner's scope and incentive structure were not designed to own the custom engineering layer. The work fell to the internal IT team, which was already at capacity managing the implementation program itself.
The third was treating data governance as a pre-migration deliverable. The organizations that arrived at cutover with clean, consistently mapped, legally defined patient records had made that investment 12 to 18 months before go-live as a prerequisite to starting one. The programs that deferred data governance discovered mid-program that they lacked both a consistent trusted data source and a clearly defined legal medical record.
None of these approaches required a larger budget at program kickoff. They required earlier recognition that the Implementation Boundary is a program and that it needs an owner before the EHR vendor's implementation clock starts running.
"Ideas2IT provides EHR data migration services specifically scoped to the Implementation Boundary the engineering layer that EHR vendors and implementation consultants both stop short of. The Implementation Boundary needs an engineering team that is accountable to the health system's go-live date, embedded in the health system's existing environment, and scoped specifically to the custom data infrastructure layer. That is the engagement model Ideas2IT runs in Cerner-to-Epic programs.
Health systems that scope Implementation Boundary work as a parallel engineering program before the implementation contract is signed do not encounter it as a change order six months in. That is the operational difference the engagement is designed to produce. Ideas2IT's healthcare engineering's Forward Deployed Engineers embed in the health system's existing environment at program kickoff and deliver four specific outputs in the first 30 days: a full inventory of every custom HL7 interface mapped against the go-live cutover window, a complete CCL report extraction triaged by business owner and operational dependency, a data pipeline assessment mapped to Epic's data model with re-engineering scope defined, and a SMART app certification status review against the Oracle DSTU2 deprecation deadline. Those four deliverables define the Implementation Boundary before the implementation partner's build phase begins, when the scope can still be sequenced and resourced without compressing the go-live date.
Consult with our data migration specialists on when you should consider a cerner to epic migration for your specific usecase.