Three months ago, the RPM program worked. At that time 50 patients were on the system with one condition pathway and one EHR site. The per-patient SaaS fee looked manageable against CMS reimbursement although the alert queue was noisy but navigable.
At 300 patients, the same program looks different. The monthly SaaS invoice has reached a number your CFO has flagged. The Epic sync broke six weeks ago after an upgrade cycle your vendor did not anticipate and the fix is still pending.
What a production-grade RPM program requires at 300, 500, and 1,000 patients is a different architecture.
By 2030, over 142 million US patients, nearly 40% of the population will be using some form of RPM technology.
That growth creates a specific pressure. Programs that piloted successfully at 50 patients are being pushed to scale to 300, 500, and beyond. But the platforms selected for the pilot were not designed for that operating environment.
These three failure modes account for most RPM program breakdowns at scale.
Off-the-shelf RPM vendors price on a per-patient monthly basis. At 50 active patients, this model absorbs the vendor's development cost and leaves viable margins.
At 200 patients, monthly SaaS fees reach $10,000–$20,000 against CMS revenue potential of $29,400–$41,000. At 500 patients, fees reach $25,000–$50,000 against revenue potential of $73,500–$102,500.
The SaaS cost is now consuming a material portion of reimbursement with no path to optimization, because the buyer does not own the infrastructure.
*These are directional industry estimates. Actual break-even depends on condition mix, CMS code capture rate, and payer composition. The cost math section covers this in detail.
Every off-the-shelf RPM vendor claims Epic and Cerner integration. That claim is accurate for a single site under controlled conditions.
It does not describe the production reality of a multi-site rollout or a post-upgrade cycle.
Epic's SMART on FHIR R4 implementation requires per-site configuration, a separate security review, and a dedicated go-live activation for each deployment. The core integration codebase is reusable. The site-specific work is not.
When Epic releases an upgrade cycle, integrations built on the vendor's abstraction layer break on the vendor's timeline.
Oracle's own developer documentation confirms Cerner DSTU2 FHIR APIs reached end-of-support in December 2025, with all integrations required to migrate to FHIR R4. Any RPM platform still running legacy Cerner integrations after that date is operating non-compliant infrastructure.
Buyers who did not own their integration layer discovered this exposure after the fact.
A 2024 study published in the Journal of the American Medical Informatics Association found that 49% of RPM alerts are false positives, and that clinicians receiving more than 100 alerts per day develop measurable cognitive desensitization.
Threshold-only alerting, a single-reading breach of a static threshold was designed for low-volume, high nurse-to-patient ratio environments.
At 300 patients across a standard care team, it generates an alert volume that cannot be triaged reliably. The signals that matter arrive in the same channel as the signals that do not. Within weeks, the nursing team stops treating the alert queue as a clinical instrument.
This is described as a clinical adoption problem. It is an engineering architecture decision that requires an engineering fix.
Off-the-shelf RPM is not the wrong choice in every situation. At fewer than 200 active patients with a single condition pathway and a single EHR site, the vendor model often leaves workable margins.
The decision changes when four conditions are present.
At this threshold, the per-patient fee model becomes economically irrational for most program configurations. A custom platform carries no per-patient fee from the first patient enrolled and for most programs at this volume, the build cost amortizes within the first year of operation.
At this threshold, per-patient SaaS fees begin consuming reimbursement margin with no path to optimization because the buyer does not own the infrastructure.
Any RPM program operating across more than one EHR platform cannot rely on a vendor's single-integration architecture.
A health system running Epic for inpatient and athenahealth at referring practices needs bidirectional data in both systems. A home care program involving the ordering physician's EHR and the home health agency's platform faces the same requirement.
No off-the-shelf vendor resolves this cleanly. Custom integration engineering is the only path to reliable data flow in both directions.
Off-the-shelf vendors build for the most common use cases: hypertension, heart failure, COPD, diabetes.
A program expanding into oncology, post-surgical monitoring, or behavioral health will hit the limits of pre-built protocol templates within the first 60 days of that expansion.
Custom workflow logic is not optional at multi-specialty scale and it is what allows the program to adapt to clinical reality rather than requiring clinical teams to adapt to the software.
Home care RPM operates on a different set of engineering assumptions than hospital or ambulatory RPM.
A platform built for acute and ambulatory settings will fail in home care because the deployment context it was designed for does not exist in a patient's home.
The five requirements that differentiate home care RPM are covered in full below.
Each module below is described by the production problem it resolves. A custom RPM platform that omits or underbuilds any one of them will encounter the failure mode it was intended to prevent.
Without a clinical workflow engine covering enrollment through EHR write-back, clinical staff operate two parallel systems. Documentation falls to manual entry, and so the RPM platform becomes a monitoring tool bolted onto existing workflows rather than replacing them. The workflow engine is what converts the platform from a device dashboard into operational infrastructure.
A workflow engine covers four operational domains:
Manual documentation is a signal that the workflow engine was not built for the full operational scope of the program.
Epic uses SMART on FHIR R4 with OAuth2 strict authentication. Per-site configuration is the operational standard. Each site requires separate configuration, security review, and go-live activation.
Cerner uses Ignite APIs with FHIR R4 now required since the DSTU2 deprecation in December 2025. [10]
Athenahealth covers home care and home health agency connectivity, where its simpler FHIR implementation is consistently overlooked by platforms built for health systems.
For multi-EHR deployments, the FHIR Facade Pattern, a single standardized API layer translating to vendor-specific APIs normalizes data structures across Epic, Cerner, and athenahealth without rebuilding integration logic per site.
For a deeper look at how hospitals are building owned FHIR integration infrastructure, see Custom FHIR Integration Hub Development for Hospitals.
Without device-agnostic ingestion, every new device manufacturer requires a new ingestion build.
Without cellular-native support and transmission buffering, a gap from a home care patient's device becomes a data void which means either erroneous alerts or holes in the monitoring record.
This layer normalizes data from multiple device manufacturers like blood pressure cuffs, scales, pulse oximeters, glucose monitors without rebuilding ingestion logic per device.
In home care, cellular-native device support with buffering and retry logic is a hard architecture requirement.
Without a triage architecture replacing threshold-only alerting, alert volume at 300+ patients produces the clinical behavior described in the opening section: nursing teams that stop treating the queue as a clinical instrument.
The six-layer triage architecture that replaces threshold-only alerting:
Industry implementations of this architecture report 60–80% alert volume reduction while maintaining sensitivity for genuine deterioration events.
Without automation for all seven active codes including CPT 99445 and 99470, which most commercial vendors had not integrated by their January 2026 effective date revenue is leaking on every patient whose monitoring pattern qualifies for the new codes.
The 2026 Physician Fee Schedule finalized two new CPT codes effective January 1, 2026:
Both codes fill gaps the prior 16-day threshold and 20-minute threshold requirements left uncompensated. Most commercial vendors had not fully integrated either code as of the January 2026 effective date.
A custom billing module must support all seven active codes, including automated time tracking and audit trail generation for the live synchronous communication requirement that governs 99457 and 99470.
Text messages and voicemail do not qualify.
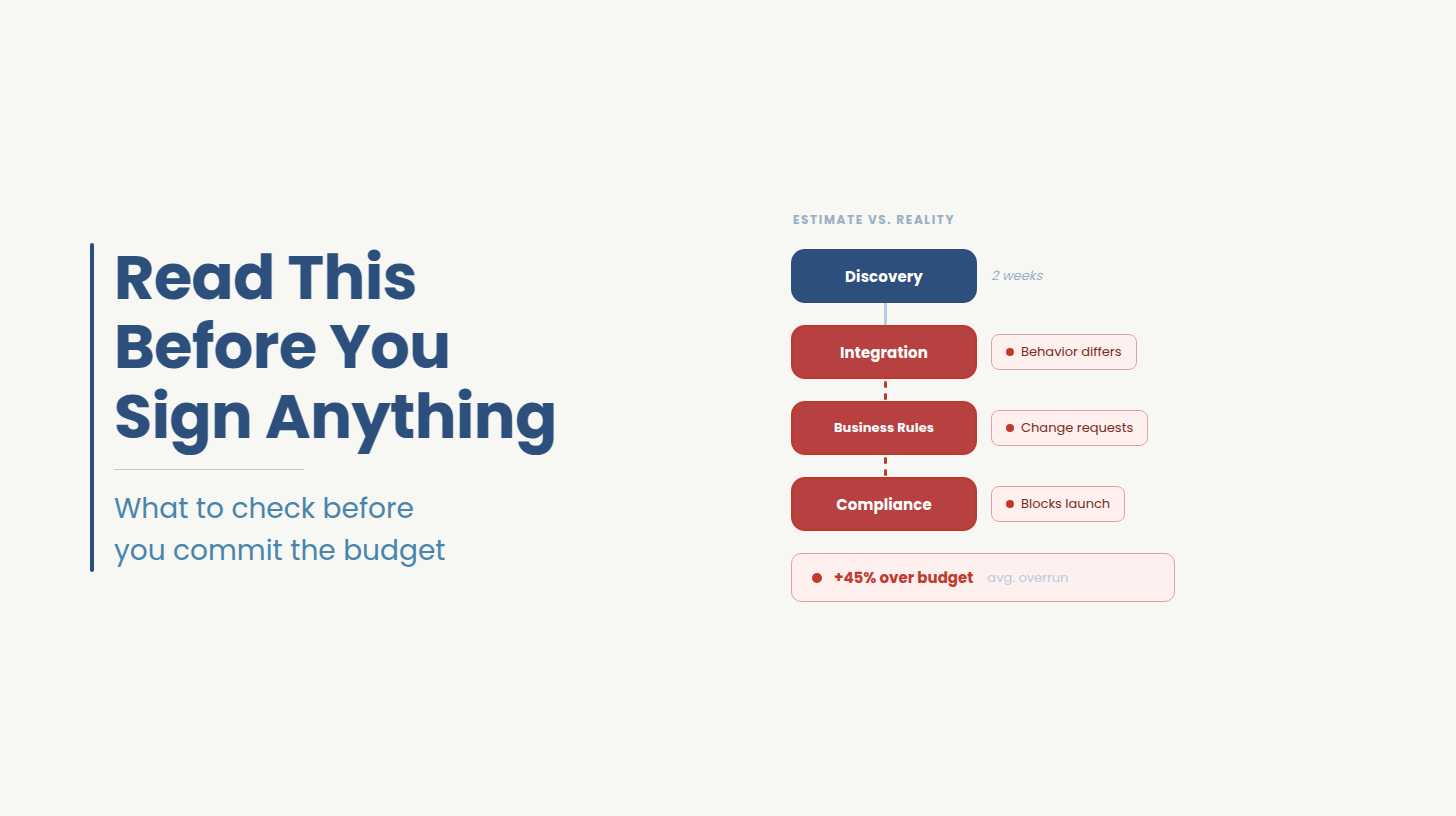
A custom RPM platform costs $80,000–$130,000 for an MVP covering one condition pathway and a single EHR integration, delivered in four to five months. A full production platform covering multiple specialties, multi-EHR integration, AI alert triage, and seven-code CMS billing automation costs $150,000–$350,000 over nine to eighteen months. Break-even against CMS reimbursement occurs at approximately 200 active patients for most configurations.
The $150,000–$350,000 build figure is the wrong number to anchor on. The relevant calculation is the per-patient break-even against CMS revenue.
*SaaS fee ranges and custom build cost ranges are directional industry estimates. CMS revenue figures are based on conservative code capture. Actual break-even depends on condition mix, payer composition, and billing team capacity.
At 500 patients with full capture of all seven codes, CMS revenue potential reaches approximately $101,500 per month. A custom platform with no per-patient fee amortizes a $300,000 build cost in approximately three months of operation.
The build decision is a business arithmetic question.
If you want to run this math against your actual patient volume and CMS code capture rate, the $0 scoping session produces a break-even model calibrated to your program.
Book a session →
Seven CPT codes are active for RPM billing in 2026. The 2026 Physician Fee Schedule added two new codes effective January 1: CPT 99445 covering device supply for 2–15 monitoring days at approximately $52, and CPT 99470 covering the first 10 minutes of care management at approximately $26. Both codes remain unintegrated in most commercial RPM platforms as of mid-2026.
Rates sourced from thoroughcare.net's March 2026 analysis and Nixon Law Group's February 2026 review of the 2026 CMS final rule.
Post-discharge patients frequently do not reach the 16-day transmission threshold required for CPT 99454. CPT 99445 covering device supply for 2–15 monitoring days was specifically designed for this scenario, and home care organizations running post-discharge programs are its primary beneficiaries. Most commercial vendors had not integrated 99445 into their billing modules as of its January 2026 effective date.
At 200 monthly post-discharge patients, the revenue gap from uncaptured 99445 claims is not a minor billing adjustment. It is a material revenue loss on every patient who transmits for fewer than 16 days. A custom billing automation module built to capture 99445 from go-live recovers that revenue from the first patient enrolled.
Is your RPM program approaching the break-even threshold?
Ideas2IT offers a $0 scoping session to spec your RPM build before you spend a dollar on development. In 90 minutes, you walk away with a break-even model calibrated to your actual patient volume and CMS code capture rate, plus a feature-level build specification you own regardless of next steps.
Book a $0 RPM Scoping Session →
Home care and hospital-at-home deployment has grown into the highest-volume RPM expansion area in 2026, driven by decentralized care and post-discharge readmission prevention programs.
Off-the-shelf platforms built for acute and ambulatory settings underserve this context across five specific requirements.
Home care patients cannot be assumed to have reliable Wi-Fi.
Devices must be cellular-native with blood pressure cuffs, scales, pulse oximeters, and glucose monitors that transmit directly over 4G/LTE without requiring a smartphone or home hub.
The platform must handle transmission gaps with buffering and retry logic. A cellular-first architecture is not a device procurement requirement. It is a software architecture requirement for how the platform handles inconsistent transmission.
Hospital RPM operates on real-time bedside alert streams while home care does’nt.
Home care operates on a scheduled cadence, a clinical team reviews batched vitals windows. Alert logic designed for real-time hospital monitoring fires on single-reading threshold breaches against a 24-hour data set that was never intended to support that model.
The result is immediate alert fatigue. Alert logic must be designed for 24–72 hour trend windows and deterioration patterns.
A home care RPM program involves two distinct systems: the ordering physician's practice EHR (Epic, athenahealth, or Charm Health) and the home health agency's own EHR or care management platform.
RPM data must appear in both workflows for clinical and billing purposes. No off-the-shelf vendor solves this cleanly.
Bidirectional FHIR R4 integration to both systems is the engineering requirement and it is the reason athenahealth must be part of the integration plan even when the health system runs Epic.
The primary home care RPM use case is readmission prevention during the 30-day post-discharge window.
The platform must automate physician order generation at discharge, device logistics coordination, home health nurse training handoff, and enrollment activation. Without automation at each step, a program running 200 monthly discharges requires a manual coordination load that eliminates the clinical capacity the RPM program was designed to create.
For context on how custom workflow software addresses home care operational gaps, see Custom Patient Intake and Scheduling Software: A CTO's Build Decision Guide.
Post-discharge patients frequently do not reach the 16-day transmission threshold required for CPT 99454.
The 2026 code 99445 covers device supply for 2–15 monitoring days, specifically designed for this scenario. [4] Home care organizations running post-discharge programs are the primary beneficiaries.
Most commercial vendors had not integrated 99445 into their billing modules as of its January 2026 effective date which means home care programs on off-the-shelf platforms are leaving reimbursement uncaptured on every post-discharge patient who transmits for fewer than 16 days.
A home health technology company engaged Ideas2IT to replace a manual home care workflow from intake and scheduling through care plan documentation and claims filing with a HIPAA-compliant mobile EHR. Clinicians gained real-time access to treatment plans, patient vitals, and medications on any device at point of care. The outcome: simplified data entry, improved caregiver experience, and reliable connectivity across a distributed home care workforce operating where connectivity could not be assumed.
Every off-the-shelf RPM vendor claims EHR integration. The table below documents what that claim means in production across the three EHR platforms that account for the majority of US health system and home care deployments.
The FHIR integration layer is the most technically complex component of a custom RPM platform and the source of most production failures in vendor-originated deployments. Enterprise multi-EHR integration ranges from $50,000 to $500,000 depending on scope, number of sites, and integration depth required.
HIPAA compliance in an RPM platform is not a post-build audit. It is a set of engineering decisions made at the architecture stage.
PHI encryption applies to every data path from device to platform to EHR. Every cellular transmission, every FHIR resource, every data store that touches a patient record requires encryption at the appropriate layer. A BAA with the RPM platform vendor alone is not sufficient, the chain must extend to device manufacturers and cellular carriers in the data path.
Audit logging for time-based CPT codes is a billing requirement, not just a compliance one. CPT 99457, 99470, and 99458 require documented proof of live, synchronous interactive communication: date, method, staff member, and cumulative minutes per period. Text messages and voicemail do not qualify. [9] Missing or manually entered logs mean denied claims.
Role-based access controls clinician, care coordinator, billing team, administrator must be configured at the build stage. A single-role access model creates compliance exposure and operational risk, particularly in home care programs where the care team spans multiple organizations.
A custom RPM platform is not an 18-month project before value is realized. A phased delivery model produces clinical and billing value at each milestone.
Phase 1: Discovery and architecture (4–6 weeks)
Input: EHR environment mapping, device ecosystem assessment, condition pathway scoping, billing team workflow documentation, and alert escalation protocol definition.
Output: an architecture specification that governs every subsequent build decision.
Programs that skip this phase typically redo it in the middle of Phase 2 at a higher cost.
Phase 2: MVP platform (4–5 months total, $80K–$130K)
One condition pathway, bidirectional EHR integration for the primary EHR site and cellular-native device ingestion with Basic alert logic.
CPT 99453, 99454/99445, and 99457/99470 billing automation with first patient enrolled at the end of Phase 2. And here the per-patient fee clock stops at go-live.
Phase 3: Production platform (9–18 months total, $150K–$350K)
Multi-specialty condition pathways including multi-EHR integration with the FHIR Facade Pattern.
IoMT device-agnostic ingestion with six-layer AI alert triage and full 7-code billing automation. A program entering discovery in Q3 2026 can have its first patient enrolled on a custom platform before the end of Q4 2026.
Ideas2IT works with health systems and digital health companies in two configurations.
Fixed-scope project delivery for organizations that need a defined output with a defined timeline. Embedded engineering teams for organizations that need ongoing platform ownership, EHR upgrade cycles, new CMS code integration, alert threshold governance because those are continuous engineering problems.
Most RPM engagements begin as fixed-scope for the MVP phase and transition to embedded for production platform ownership.
Before writing a line of code, the engineering team maps the existing environment: EHR stack, clinical workflow systems, billing team's current process, device ecosystem, and the care team's alert escalation protocol.
This is an architecture session. The output is a specification that governs every subsequent build decision. From that specification, the engagement runs in the three phases described above.
Ideas2IT's Anticlock platform governs the AI-native SDLC layer of this ongoing ownership: converting new requirements like a 2027 CMS code change, a new EHR upgrade cycle, a new alert threshold protocol into sprint-ready architecture with senior-engineer guardrails. The delivery risk of ad-hoc sprint work against a live clinical platform is the risk Anticlock is designed to eliminate.
Here’s what makes Ideas2IT the preferred partner for custom RPM builds
Most development partners can integrate Epic in a controlled environment. The production reality with per-site configuration variability, OAuth2 strict authentication, rate limits at ten requests per second per OAuth token, upgrade cycles that break integrations on the vendor's timeline requires engineers who have been through that cycle on live deployments.
The same applies to Cerner's DSTU2 deprecation in December 2025, which exposed every RPM platform running legacy integrations after that date. Ideas2IT builds integration layers the client owns. Upgrade cycle exposure belongs to the engineering team
Generalist development firms hire a healthcare consultant to translate clinical requirements into engineering specs. The translation layer introduces errors and delays.
At Ideas2IT, the engineers working on the alert triage architecture understand why threshold-only alerting fails at 300 patients. The engineers building the billing module understand why CPT 99457 requires documented live synchronous communication and why a text message does not qualify. Clinical workflow logic is understood by the people building it instead of handing it over as a requirements document.
A US-based development firm building a comparable RPM platform at the same engineering depth costs two to three times more for the same scope. The offshore cost advantage does not come at the expense of healthcare regulatory knowledge like HIPAA architecture, CMS billing accuracy, FDA software classification awareness because that knowledge is built into the team.
For a $300,000 build that amortizes in three months at 500 active patients, the cost structure is what makes the build decision rational in the first place.
In a scenario where CMS adds two new RPM codes or epic releases an upgrade cycle and a new specialty pathway needs a condition protocol, these are not edge cases. They are the operational reality of running RPM as a permanent care delivery program.
An engagement model that ends at go-live means rebuilding the vendor relationship every time the regulatory or technical environment changes. The embedded team model means the engineering team that built the platform owns its ongoing evolution as co-owners of the production environment.
As part of its healthcare software development services, Ideas2IT has delivered HIPAA-compliant healthcare platforms across home care, chronic disease management, and clinical workflow automation including a mobile EHR for a distributed home health workforce that automated the full operational chain from patient intake through claims filing giving clinicians real-time access to treatment plans, vitals, and medications at point of care across a workforce where connectivity could not be assumed.
For RPM-specific deployments, the engineering stack covers FHIR R4 bidirectional sync across Epic, Cerner, and athenahealth; cellular-native IoMT ingestion; the six-layer alert triage architecture; and CMS billing automation for all seven active CPT codes including the 2026 additions.
Ideas2IT holds AWS Healthcare Competency certification, SOC 2 Type II, and ISO 27001, and operates HIPAA-compliant infrastructure across all healthcare engagements.
Your RPM program has passed the threshold where the current architecture is creating constraints your vendor cannot resolve.
Per-patient fee structures with no optimization path, integration layers you do not own, and alert architectures not designed for your patient volume these are engineering problems with engineering solutions.
A 60-minute scoping session with the Ideas2IT team produces four concrete outputs:
[1] MarketsandMarkets, Remote Patient Monitoring Market Report 2025–2030, https://www.marketsandmarkets.com/Market-Reports/remote-patient-monitoring-market-77155492.html
[2] MarketsandMarkets, Remote Patient Monitoring Market Report 2025–2030 (North America share and software CAGR), same source as [1]
[3] thoroughcare.net, 2026 Remote Patient Monitoring CPT Codes: 99470, 99457, 99453 and more (March 2026), https://www.thoroughcare.net/blog/remote-patient-monitoring-billing-rules
[4] Nixon Law Group, CMS Finalizes 2026 Remote Monitoring Reimbursement Updates (February 2026), https://www.nixonlawgroup.com/resources/cms-finalizes-2026-remote-monitoring-reimbursement-updates-what-changed-for-rpm-and-rtm
5] Oracle Health, DSTU 2 Overview, Millennium Platform APIs, https://docs.oracle.com/en/industries/health/millennium-platform-apis/mfdap/dstu2_overview.html
[6] Journal of the American Medical Informatics Association (2024), cited in nirmitee.io, RPM Alert Fatigue: Why Clinicians Ignore 70% of Remote Alerts, https://nirmitee.io/blog/rpm-alert-fatigue-clinicians-ignore-70-percent-alerts-ai-fixes/
Didn't find what you were looking for?