Most telehealth platforms in production today were built between 2020 and 2022. They were built fast under clinical pressure, with minimal EHR integration, compliance scoped for basic HIPAA, and no architecture for the AI capabilities that were three years away. At the time, that was the right call. Patients needed access. Providers needed tools. Speed was the only metric that mattered.
In 2026, those same platforms are the single biggest obstacle to what health systems are now being asked to deliver. Ambient clinical documentation requires EHR write-back capability that most 2021 builds do not have. AI triage requires real-time patient data flows that surface-level FHIR connections cannot support. Multi-state prescribing requires compliance architecture that was never scoped. Enterprise procurement now requires SOC 2 Type II that was never built.
Meanwhile, physicians already spend two hours on EHR documentation for every one hour they spend with patients [2] a burden that compounds when the telehealth platform cannot feed ambient AI tools
The 2021 platform is not aging gracefully. It is actively blocking clinical and operational priorities that your CMO, your compliance team, and your health system partners are already tracking.
Before any conversation about architecture, timelines, or vendors, it is worth being precise about which situation you are actually in. The right response to each one is different. The questions you need answered before making a decision are different. And the risk of choosing the wrong path is significant in all three.
SITUATION A
The Rebuild That Stalled
What you’re experiencing: You started upgrading or replacing the platform. EHR integration became the bottleneck at month three. The vendor who said six months is now asking for another sprint. The board is asking questions you cannot answer with specifics.
Root cause: The vendor quoted EHR integration as a single line item without a milestone-based timeline. They had not completed Epic App Orchard certification before. The discovery phase the work that should have happened before the contract is happening inside your budget.
SITUATION B
Live But Structurally Stuck
What you’re experiencing: The platform works. Patients use it. But your CMO wants AI triage by Q3. Your compliance team wants SOC 2 by year end. Your EHR team says the current architecture cannot support write-back for ambient documentation. Every new requirement reveals a structural limitation that was baked in during the original build.
Root cause: The 2021 build optimized for launch, not for the platform’s second and third year. The decisions that felt safe in 2020 commercial SDK for video, read-only FHIR, single-state compliance are now the ceiling on what the platform can become.
The operational consequence: 77% of physicians report that excessive documentation tasks lead to longer clinic hours or work from home. [3]Up to 75% of physicians with burnout symptoms identify the EHR as the source. [4]A platform that cannot support ambient documentation is not just a technical liability. It is a physician retention risk.
SITUATION C
New Build, Paralyzed by Vendor Proposals
What you’re experiencing: You know the current platform is a liability. You have three vendor proposals. Prices vary by $200K and nobody can explain why. You cannot tell which vendor has actually done EHR integration at depth versus which one has mentioned FHIR in a slide deck.
Root cause: Vendor proposals are scoped to what the buyer asks for, not what the build actually requires. Without a framework to evaluate what is behind the numbers, every proposal carries the same risk. You are not comparing like for like because no two vendors are quoting the same scope.
All three situations above trace back to the same architectural decisions made at the start of most telehealth builds in the 2020–2022 period. Understanding them is what allows you to evaluate whether remediation is viable or whether a rebuild is the more defensible choice.
Commercial video SDKs like Twilio, Daily.co, Vonage were the rational choice in 2021. They ship in weeks, handle HIPAA BAA requirements, and manage scaling infrastructure. The problem is not what they do. The problem is what they prevent.
Ambient clinical documentation requires hooks into the video layer that commercial SDKs do not expose. Multi-party specialist routing requires call orchestration control that sits below the SDK abstraction. AI-powered quality monitoring and real-time transcription with clinical write-back require access to the raw media stream. Health systems that selected commercial SDKs in 2021 for speed are now discovering that the features clinical leadership is requesting in 2026 require control over the video infrastructure that the SDK does not allow.
Over 95% of U.S. hospitals use a certified EHR platform [5] yet most run separate systems for doctors, labs, radiologists, and remote monitoring devices with incompatible data formats. Having an EHR and having EHR integration are two different things.
Most 2021 telehealth builds either skipped EHR integration entirely for the MVP or implemented read-only data pulls via FHIR enough to pre-populate a patient record on a call, not enough to write clinical output back into the EHR. At the time, that was a reasonable scope decision.
In 2026, ambient documentation requires write-back. AI triage requires real-time access to the patient’s full clinical history, not a summary pulled at session start. RPM integration requires continuous bidirectional device data flow. A platform with read-only FHIR connectivity cannot support any of these without rearchitecting the data layer which in practice means rebuilding the data foundation of the application.
Ideas2IT uses LegacyLeap’s agentic discovery engine to assess existing EHR integration architecture in under one week replacing the 6–8 week manual assessment that most remediation engagements begin with. For health systems in Situation B or A, this is the tool that determines whether remediation or rebuild is the defensible path before a dollar is committed to either.
Basic HIPAA compliance encryption at rest and in transit, audit logging, BAA execution, access controls was sufficient for enterprise deployment in 2021. It is not sufficient now. Enterprise health system procurement in 2026 requires SOC 2 Type II, multi-state telehealth prescribing architecture, and DEA EPCS compliance for e-prescribing. These are not add-ons that can be applied to an existing platform. They require architectural decisions about data handling, audit log structure, and access control that must be made at the foundation level.
Health systems attempting to add SOC 2 Type II to a platform not designed for it consistently discover that the audit logging requirements alone require changes to the data architecture. The compliance layer was always a foundation decision.
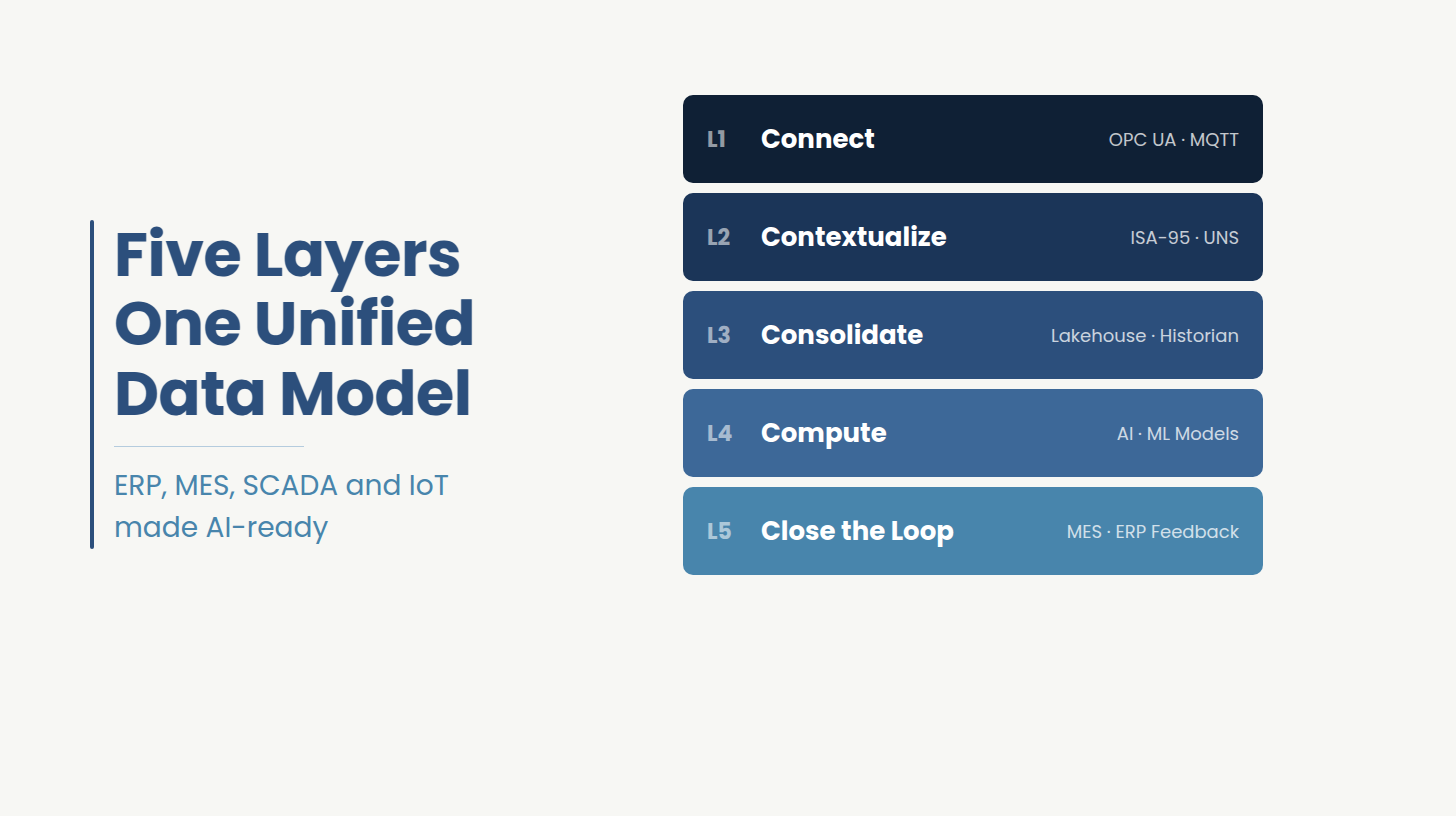
Whether you are evaluating a remediation of your existing platform or commissioning a new build, the following five architecture layers are non-negotiable for enterprise deployment in 2026. Each one is also a vendor evaluation criterion: a development partner who cannot speak specifically to each of these has not built a production-grade telehealth platform.
The evaluation question is whether the vendor supports FHIR and at what level of integration they have completed in production: read-only data pulls, bidirectional scheduling, or full clinical write-back including ambient documentation output and AI-generated notes.
For Epic: App Orchard registration, FHIR API development, sandbox testing, and a certification review process. Budget $60K–$120K and four to six months. For Cerner: $40K–$80K, three to five months. For Athena: $30K–$60K, two to four months. A vendor who cannot quote these as separate line items with milestone-based timelines has not completed them.
The right video infrastructure decision depends on three variables: projected visit volume at month 12 and month 36, the AI feature requirements for the video layer, and the organization’s tolerance for infrastructure management overhead. A development partner who recommends the same approach regardless of these variables is optimizing for their workflow.
Commercial SDKs (Twilio, Daily.co) are cost-effective below approximately 800K monthly minutes and appropriate when AI hooks are not required. Open-source WebRTC is the correct choice when ambient documentation, multi-party routing, or AI monitoring are in scope. The decision made at kickoff creates a per-visit cost structure that persists for the life of the platform.
SOC 2 Type II, multi-state prescribing law architecture, and DEA EPCS compliance cannot be retrofitted into a platform designed without them. These requirements must be scoped at the architecture level before a line of code is written. A proposal that places compliance on the roadmap rather than in the foundation is a proposal that will require rearchitecting.
The global AI in telehealth market reaches $5.64 billion in 2026 and is growing to $32.18 billion by 2034 at a 24.31% CAGR [6] — and 62% of healthcare systems have already integrated AI into telehealth operations. [7] These are no longer emerging capabilities. Health systems that have not adopted them are operating below the adoption midpoint.
Ambient clinical documentation, AI triage, async care workflows, and RPM device integration are now appearing as enterprise procurement requirements, not roadmap aspirations. All four require specific architectural decisions at the platform foundation.
Every capability in the table above requires EHR write-back integration to function in a clinical environment. A platform without production-grade bidirectional EHR integration cannot support any of them.
Epic and Cerner release API updates on regular cycles. A telehealth platform with active EHR integration requires ongoing engineering ownership of that integration like someone who understands the data architecture, owns the maintenance cycle, and can respond when the EHR vendor changes something upstream. A build-and-handoff vendor cannot provide this by definition. The question to ask before signing: who owns EHR API maintenance in year two, and what is the SLA?
The $40K to $300K range that appears in every telehealth development guide reflects three fundamentally different builds, not price variance on the same product. The component table below maps cost by architecture decision and names what drives the variance.
Two line items are consistently absent from initial vendor quotes: EHR integration and compliance depth. Together they consume 40 to 60 percent of enterprise-grade telehealth budgets. A quote that excludes both is not competitive pricing. It is an incomplete scope.
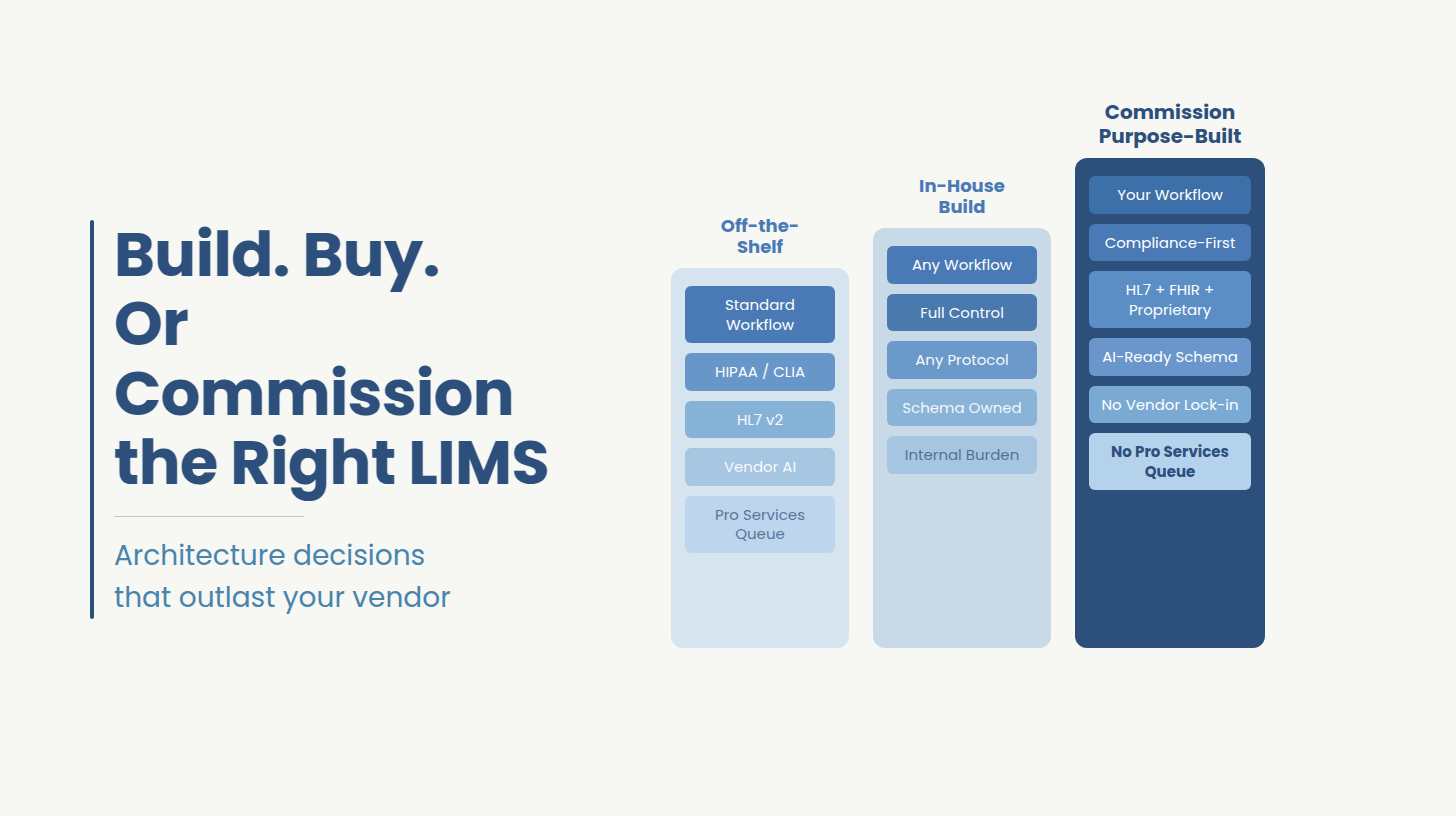
White-label telehealth platforms (Doxy.me, VSee, Amwell) cost $10 to $25 per visit with $5K to $20K in setup fees. Custom platforms cost $150K to $300K upfront with $25K to $50K per year in maintenance.
Build vs Buy Breakeven
White-label at $15 per visit, 500 visits per month: $90,000 per year ongoing.
Custom build at $200K upfront, $35K per year maintenance: $235K in year one, $35K thereafter.
Breakeven: month 26 to 28.
Below 300 visits per month: buy. Above 800 visits per month: build. Between 300 and 800: depends on whether telehealth is a product differentiator or a feature.
White-label platforms also impose an AI ceiling. Once you need ambient documentation, AI triage, or custom specialist routing, you are fighting the platform. Migration at that point costs more than building custom from the start would have.
Annual maintenance on a production telehealth platform runs 15 to 25 percent of initial development cost. On a $200K build: $30K to $50K per year before a single new feature is added. On a platform with active Epic integration, EHR API maintenance alone justifies a dedicated engineering resource. This figure is absent from virtually every development vendor’s initial proposal.
A 90-day telehealth MVP is achievable under specific conditions through the right healthcare software development partner: web-first deployment, a commercial video SDK, no EHR integration, single-state HIPAA compliance, and a feature scope limited to video consultation, scheduling, secure messaging, basic clinical notes, and payment processing. That product is useful for validation. It is not what most organizations who say ‘90 days’ actually need by the time the project is underway.
Three specific failures convert a 90-day project into a 7-month one. EHR integration is added after architecture is locked, requiring a data layer rework. Compliance scope expands post-kickoff when a health system buyer specifies SOC 2 as a procurement requirement. Platform targets change from web-first to native iOS and Android after development has started on a cross-platform framework.
None of these are unusual. All three are predictable if the initial scoping conversation surfaces them. The question to ask before kickoff: does the vendor’s discovery process surface these decisions explicitly, or does it discover them mid-sprint?
Getting inconsistent quotes for a telehealth build?
Ideas2IT’s healthcare engineering team offers a $0 scoping assessment covering architecture decisions, EHR integration requirements, and a realistic timeline for your specific build. Contact us to book a session.
Book a $0 Assessment
Ideas2IT is an AWS GenAI Specialist Partner and HIPAA-compliant engineering firm with 800+ engineers. The engagement model is Forward Deployed Engineers, engineers who embed inside the client’s existing environment from Day 0, working within the client’s stack, compliance architecture, and operational OKRs.
For health systems in Situation A: a rebuild that has stalled means the team that scoped the EHR integration owns the App Orchard certification process. There is no handoff between the engineers who designed the data architecture and the engineers doing integration testing. That handoff is where Situation A builds typically break.
For health systems in Situation B: a live platform that cannot scale, Forward Deployed Engineers embed in the existing environment and assess the remediation path before committing to a rebuild. The LegacyLeap agentic discovery engine replaces 6–8 weeks of manual architecture assessment with under one week of automated analysis. For most Situation B platforms, the answer is not a full rebuild. It is targeted remediation of the three architectural decisions above.
For health systems in Situation C: evaluating vendor proposals, the $0 scoping assessment above produces a scope document specific to your EHR configuration, your compliance requirements, and your feature roadmap. Every proposal you receive after that can be evaluated against the same baseline.
Engagement Reference
A platform serving 1,300+ community-based care organizations needed ambient clinical documentation at network scale. The existing architecture had no EHR write-back capability and a commercial video SDK that did not support AI documentation hooks.
Ideas2IT Forward Deployed Engineers embedded in the client’s existing environment, and determined that a targeted remediation was viable without a full rebuild. The engagement delivered bidirectional EHR integration with ambient documentation write-back, a migration from commercial SDK to a WebRTC layer with AI hooks, and a QA framework powered by Qadence that auto-generated 70% of regression test cases across the EHR integration scenarios.
Book a 30-minute scoping call with Ideas2IT’s healthcare engineering team covering your current platform’s architecture gaps, EHR integration requirements, and what the right build or remediation looks like for your specific situation.
Book Your $0 Assessment
[1] Toward Healthcare / Fortune Business Insights, “U.S. Telehealth Market Size, Share and Forecast to 2034.” https://www.towardshealthcare.com/insights/us-telehealth-market-sizing
[2] American Medical Association, “With Ambient AI, 93% of Doctors Can Give Patients ‘Full Attention.’” (Citing Dr. Veena Jones, Chief Medical Information Officer, Sutter Health, 2025 American Conference on Physician Health.) https://www.ama-assn.org/practice-management/digital-health/ambient-ai-93-doctors-can-give-patients-full-attention
[3] American Medical Association, “With Ambient AI, 93% of Doctors Can Give Patients ‘Full Attention.’” (Citing Dr. Veena Jones on 77% of physicians reporting excessive documentation leads to longer hours or work from home.) https://www.ama-assn.org/practice-management/digital-health/ambient-ai-93-doctors-can-give-patients-full-attention
[4] Wu Y. et al., JMIR Medical Informatics, “Evaluating the Prevalence of Burnout Among Health Care Professionals Related to EHR Use: Systematic Review and Meta-Analysis.” 2024. https://medinform.jmir.org/2024/1/e54811
[5] PMC / National Library of Medicine, “Impact of Electronic Health Record Interoperability on Telehealth Service Outcomes.” https://pmc.ncbi.nlm.nih.gov/articles/PMC8790688/
[6] Fortune Business Insights, “AI in Telehealth and Telemedicine Market Size, Share and Industry Analysis, 2026–2034.” https://www.fortunebusinessinsights.com/ai-in-telehealth-telemedicine-market-115853
[7] Global Growth Insights, “Telehealth Market Report: Virtual Consultation Adoption and AI Integration Statistics.” https://www.globalgrowthinsights.com/market-reports/telehealth-market-123323
[8] AMA / JAMA Network Open, “Sutter Health Ambient AI Pilot: Provider Experience and Documentation Outcomes.”https://www.ama-assn.org/practice-management/digital-health/ambient-ai-93-doctors-can-give-patients-full-attention