A laboratory information management system decision looks simple from the outside. Pick a platform, configure it for your workflows, go live. Most labs do exactly this. Then, 12 to 18 months later, the EHR integration still requires a manual export. A routine 21 CFR Part 11 audit returns six findings. Every workflow change goes into a professional services queue with a six-week turnaround.
The LIMS works but is just not working for the lab it was built into.This is architecture debt, a structural limit built into the system at design time that grows harder to work around as the lab’s compliance surface expands, its instrument suite grows, and its data science team starts asking for feeds the LIMS was never designed to produce.
Custom LIMS software development is routinely framed as a build-or-buy decision. That framing is too narrow and ignores a third path that most procurement conversations never reach: commissioning a purpose-built system from a qualified engineering partner. This article lays out when that path is correct, what it requires, and what architecture decisions determine whether your LIMS runs out of headroom.
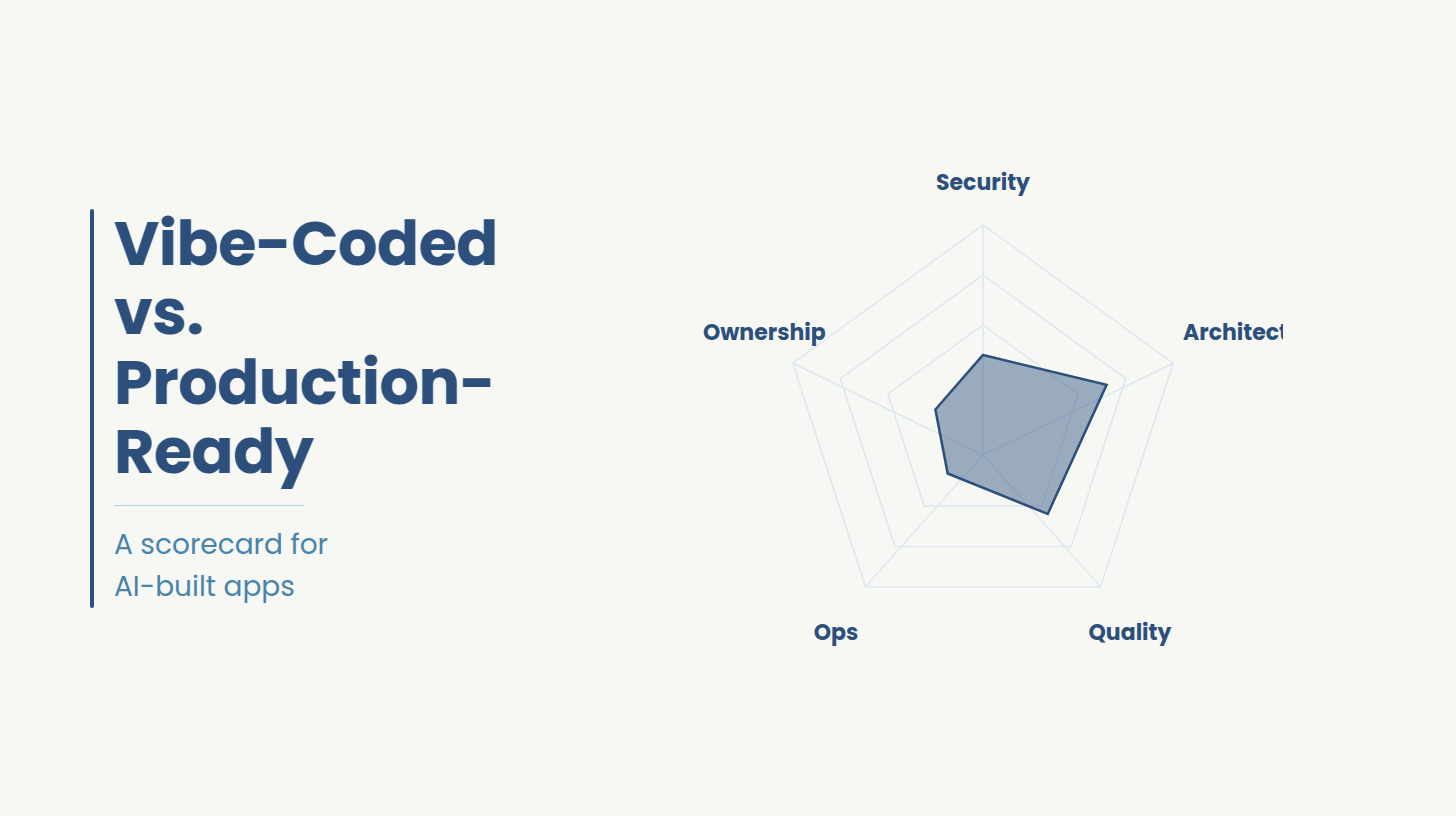
Architecture debt in a LIMS is the gap between what the system was designed to do and what the lab now requires. It is not a visible defect at go-live. It presents in three distinct operational forms, and most lab leadership teams have experienced at least two of them before they connect the pattern.
Integration friction: The EHR does not receive structured lab results. Results arrive as PDFs or manual exports, detached from clinical context. A KLAS Research study found that 68% of labs using outdated or poorly connected LIMS lose more than 20% efficiency in sample processing, experience transcription error rates above 15%, and see turnaround times delayed by more than 30%. These are architectural consequences and not just gaps.
Compliance gaps at audit: Routine audits return findings on elements the team believed were configured correctly. The audit trail does not capture the right fields. The e-signature workflow does not meet the OOS documentation standard. The system was never built around the lab’s specific compliance surface, it was configured to approximate it.
Configuration cost compounding: Every workflow customization is billable professional services. Costs multiply yet the Capability doesn't. The vendor knows the product while they do not know the lab’s processes. That gap is priced permanently into every subsequent engagement.
Off-the-shelf LIMS is architected for the median lab workflow. It works well when requirements sit close to that median. It runs out of headroom the moment they diverge: a genomics LIMS running multi-instrument pipelines, a pharmaceutical LIMS managing simultaneous 21 CFR Part 11 and ISO 17025 obligations, a multi-site CDMO with distinct reporting chains per site. The integration layer assumes standard HL7 or FHIR implementations. The compliance layer assumes standard workflows. Neither holds at the edges, and the edges of the LIMS market are exactly where complex labs sit.
Homegrown LIMS avoids the median problem but creates a different one. The system is built by the team available at build time, not the team needed for ongoing compliance validation. Key-person dependency is a structural outcome. The engineers who hold the system in depth are unlikely to be available in the same roles five years later. Validation documentation required for 21 CFR Part 11 compliance is consistently under-produced under delivery pressure. Twenty-nine percent of labs cite limited in-house expertise as a primary LIMS challenge [3]. Homegrown systems do not eliminate this problem; they internalize it.
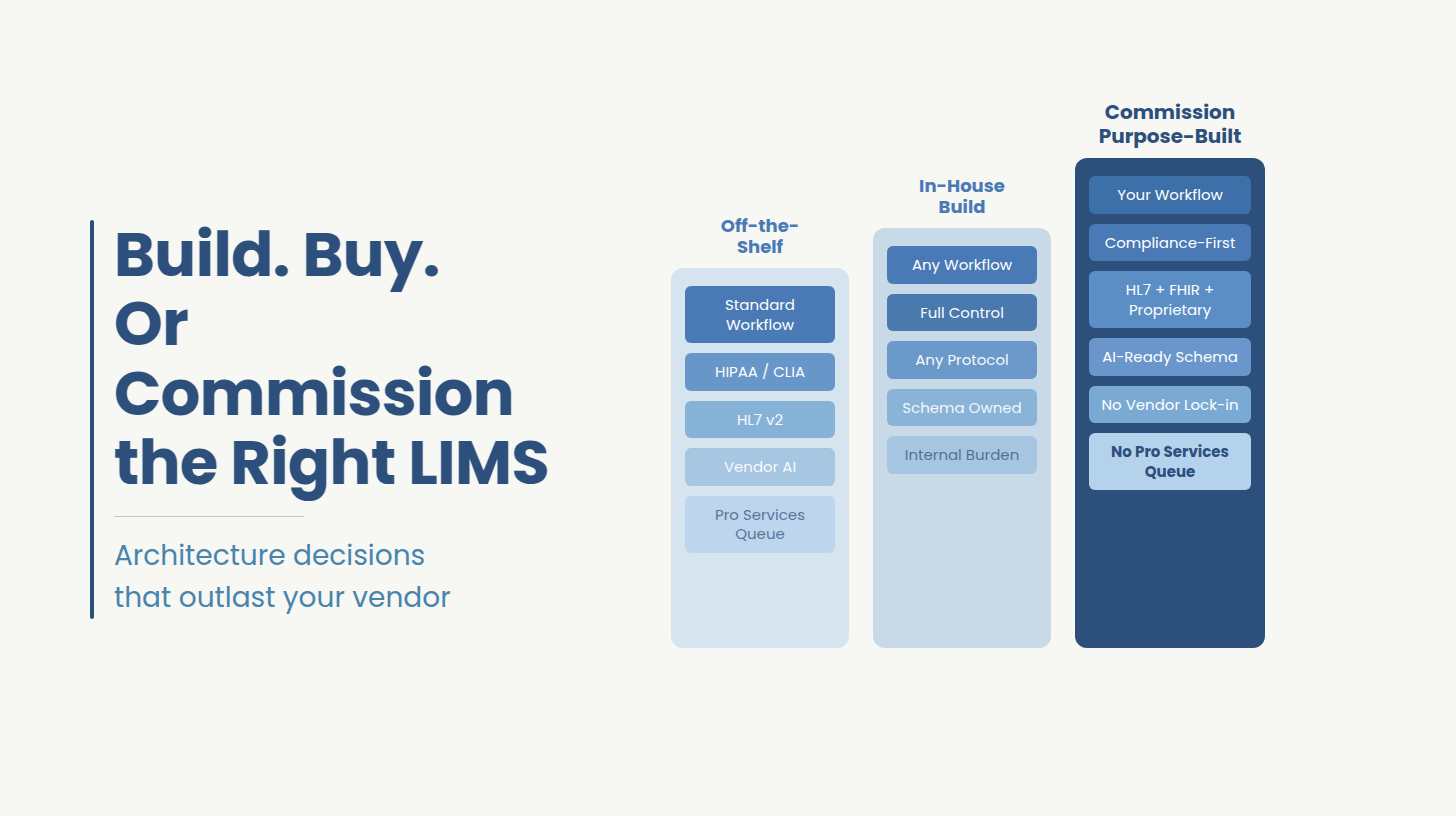
Treating the decision as binary is the error. The decision between custom LIMS vs off-the-shelf is not binary. It has three answers, and the wrong one costs two LIMS projects instead of one. Labs evaluating all three paths can review Ideas2IT's approach to custom software development before narrowing the decision.
The standard build-vs-buy question has two answers. The decision clinical and life sciences labs actually face has three. The right answer depends on five criteria specific to these environments. Here is how each path performs against them.
If the framework above surfaces gaps in your current setup, an architecture review is the right first step before a vendor conversation.
Ideas2IT runs no-cost LIMS architecture reviews that map your compliance surface, integration requirements, and AI data needs against your current system, and produce a written assessment you keep. Schedule a 45-minute session.
Schedule a scoping call
Standard off-the-shelf LIMS is built around a generalized clinical lab model. The moment a lab's workflows, data volumes, or regulatory obligations step outside that model, the configuration layer runs out of answers. Three verticals hit this ceiling most consistently.
The labs that outgrow off-the-shelf fastest are the ones growing fastest, because growth exposes every configuration workaround simultaneously.
The decision framework above shows that compliance surface is the criterion that most consistently separates what a configured system can do from what a designed system must do. Every LIMS handling clinical or pharmaceutical data operates inside at least two regulatory frameworks simultaneously. The question is where the compliance work lives: designed into the system architecture, or delegated to the lab’s manual procedures.
Each framework carries specific architectural requirements that cannot be added after the fact without rebuilding the layer they sit on.
A LIMS routing lab data through a middleware adapter rather than speaking FHIR natively is one system upgrade away from a broken LIMS EHR integration.
For labs that need an engineering partner with proven HIPAA-compliant healthcare engineering practice, the architecture decisions in this section are where that expertise is most directly tested.
The compliance gaps in the previous section and the AI readiness problem are rooted in the same architectural failure: data that is not structured, traceable, and consistently modeled at the source cannot serve either purpose well. Fewer than one-third of organizations believe their current data infrastructure is ready for AI implementation. In laboratory settings, the bottleneck is the data the LIMS produces.
Nearly 40% of lab respondents in the Pistoia Alliance 2024 survey struggled to make their data FAIR, Findable, Accessible, Interoperable, and Reusable. These are functional requirements for any AI application drawing on lab data. A LIMS that does not produce FAIR data cannot support an AI workflow without an expensive preprocessing layer between the system and the model.
The same architectural gaps that create compliance risk create the AI problem. An AI LIMS that can support predictive QC, anomaly detection, or AI-assisted result review requires four specific design decisions made at build time:
A LIMS built without these properties can still run but cannot evolve. The same architectural gap that creates compliance risk creates the AI readiness problem.
This is where architecture-by-design separates from architecture-by-configuration. Ideas2IT's engineers inherit your compliance surface before specification begins.
For labs evaluating an engineering partner with proven HIPAA-compliant healthcare engineering practice, the architecture decisions in this section are where that expertise is most directly tested.
Labs that need AI-readiness built in from day one not retrofitted at year two can start with a no-cost architecture review.
Schedule a Scoping Session
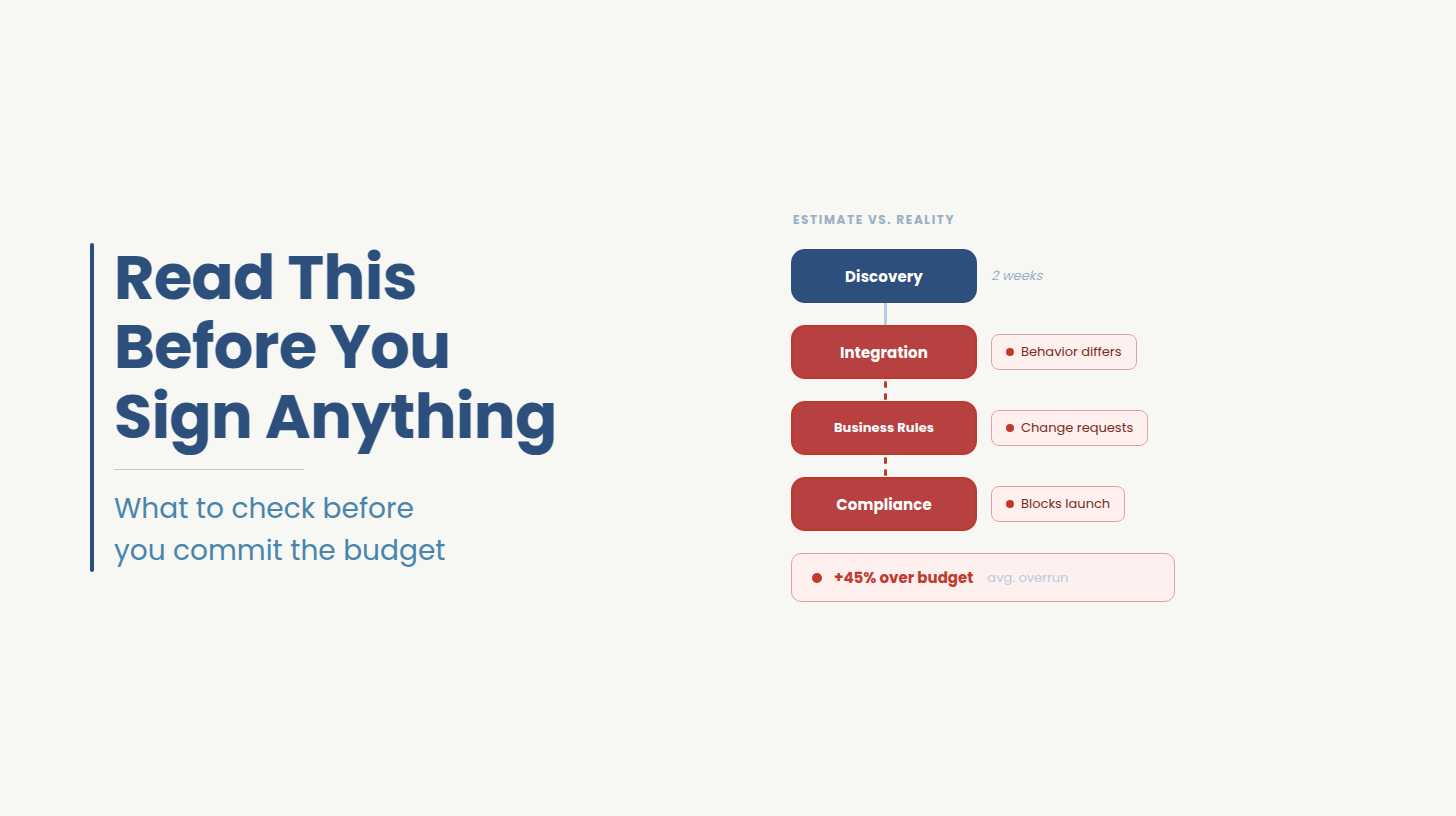
Building in AI-readiness and compliance-by-design from the start costs more in year one than a system without those properties. Understanding what drives the range is the difference between a budget that holds and one that does not.
Custom LIMS software development for a mid-to-large clinical or life sciences lab typically runs USD 200,000 to USD 1.5M, with LIMS implementation timelines of 16 to 28 weeks. The range is wide because four variables drive it significantly.
For comparison, cloud-based off-the-shelf LIMS runs USD 40 to USD 300+ per user per month in licensing, plus USD 50,000 to USD 250,000+ for enterprise-scale implementation. Professional services for workflow customization accumulate without limit on top of that.
The total cost of ownership crossover between off-the-shelf and a purpose-built custom system typically occurs before year three for labs with complex workflows and multi-framework compliance requirements. The custom build has no licensing fees and no professional services queue.
For labs with complex workflows and multi-framework compliance, the TCO crossover versus off-the-shelf typically happens before year three. No licensing fees. No professional services queue. Talk to an engineer about your environment
Most labs evaluating a LIMS development partner focus on the wrong criteria first like platform experience, team size, hourly rate. Those matter, but they do not predict whether the system will pass validation or hold up under a compliance audit two years after go-live. Four criteria do matter the most in evaluating a development partner.
Compliance-native engineering: Ask directly: does the partner design to your regulatory surface from the specification stage, or do they build the system and configure compliance on top of it afterward? The answer tells you whether audit trail schema, e-signature workflows, and access control architecture will be baked into the data model or bolted onto it. One approach produces a system that passes audit. The other produces findings.
Demonstrated HL7, FHIR, and instrument protocol experience: Generic software development shops can build a LIMS. Building one that speaks HL7 v2 and FHIR R4 natively, handles proprietary instrument data protocols without middleware adapters, and maintains bidirectional integration fidelity across EHR system updates is a different capability. Ask for specific integrations they have built and the instrument manufacturers they have worked with.
Validation documentation as a deliverable: IQ, OQ, and PQ documentation assembled retroactively after system build is the most common source of Part 11 audit findings in custom LIMS environments. The partner's delivery process should produce validation evidence alongside code at each sprint, so the documentation describes what the system actually does at every stage.
A post-go-live model that does not require a new project engagement. When your workflows change, you should not need to initiate a new vendor contract, re-scope a project, and wait for a delivery queue. The engineering team that built the system should be available to extend it under the same engagement structure, without a professional services queue and without renegotiating terms.
Ideas2IT's LIMS engineering practice is built around these four criteria. The engagement starts with a free architecture review one session that maps your compliance surface, integration requirements, and current system gaps, and produces a written assessment you keep regardless of what you decide next.
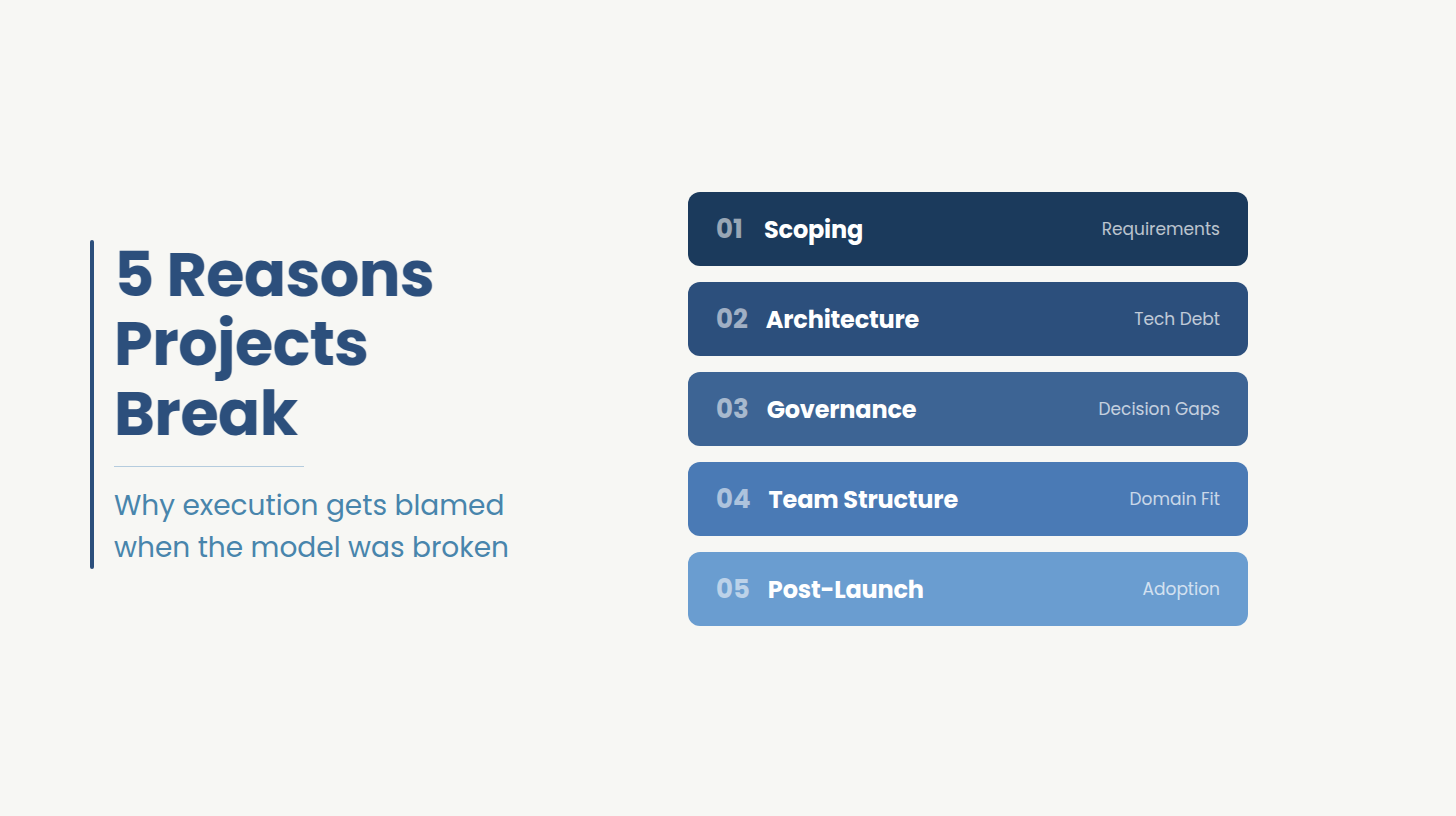
Most LIMS projects that run over budget, miss compliance at audit, or require a second implementation within three years share a root cause: the engineering team building the system did not live inside the lab’s compliance requirements, instrument architecture, and data workflows from the start. They were handed a requirements document and worked from it.
Ideas2IT builds custom LIMS differently. The delivery model, the platform tooling, and the engagement structure are all designed around one principle: the engineers doing the work must understand the environment they are building for at the same depth as the engineers who will operate what they build.
Ideas2IT does not staff a project team and hand off code. Forward Deployed Engineers embed inside the client’s environment from day one. They join the lab’s existing standups. They work within the client’s OKRs. They inherit the compliance surface, instrument integration map, and data architecture as operational context, not as a document to read.
The difference this makes is most visible at integration. Consider a lab running three instrument manufacturers, each with a different data protocol, feeding results into two separate EHR systems with different HL7 implementations. A project team working from a requirements document will map the connections as specified. An FDE working inside the lab will discover within the first two weeks that one instrument's protocol documentation is two versions out of date, that one EHR environment is staging, not production, and that the lab's preferred QC workflow requires a custom result status that neither EHR system exposes natively. None of those details are in the requirements document. All of them affect whether the system passes validation.
For a regulated LIMS build, this matters in a specific way. The gap between a requirements document and a compliant, production-grade system is always filled by engineering judgment: which audit trail fields to capture, how to handle out-of-spec result workflows, where the 21 CFR Part 11 boundary sits for a given instrument integration. FDEs carry that judgment from inside the client’s environment. External project teams carry it from their last engagement.
The result is a LIMS that is built to the lab’s specific compliance surface, not to a generalized template. For a lab managing simultaneous HIPAA, CLIA, and 21 CFR Part 11 obligations, that difference determines whether the system passes audit at go-live or surfaces findings six months later.
In a regulated LIMS build, validation documentation assembled after delivery is a compliance risk. Findings surface because the documentation describes what the system was supposed to do, not what it actually does.
Ideas2IT's engineering team operates on a standardized development process where Anticlock produces audit-ready validation documentation alongside code at every sprint. Every engineer on the project follows the same tooling, the same security guardrails, and the same deployment standards. The audit trail for the development process itself is repeatable and documentable.
For labs managing 21 CFR Part 11 obligations, this means the compliance evidence package is a structural output of how the system is built is not a documentation project that begins when the auditor schedules a visit. The sprint velocity outcome, at least 50% faster than teams without this standardized process, is a consequence of removing inconsistency overhead.
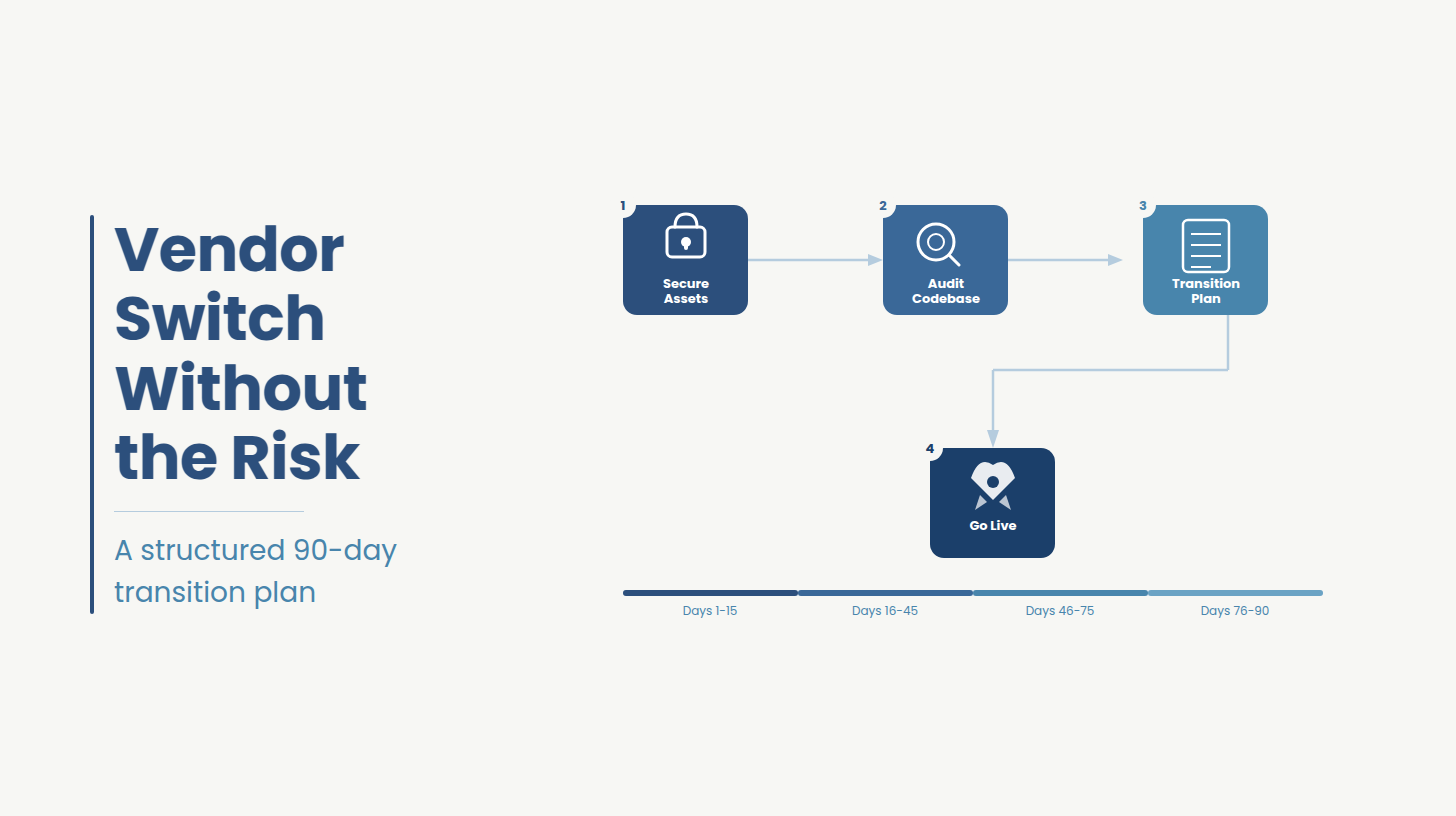
Every Ideas2IT LIMS engagement follows the same structured path from assessment to production. There are no discovery surprises billed as change orders, because the discovery work happens in the Architecture Review phase, before any build commitment is made.
The engagement model above separates Ideas2IT from the four alternatives a lab evaluating custom LIMS development most commonly considers. The comparison below shows specifically where each alternative falls short.
There are three common alternatives for a lab evaluating custom LIMS development. Here is where Ideas2IT differs from each.
For clinical lab, pharma, and biotech clients, three credentials are directly relevant to whether a custom-built system can be deployed in your environment without a separate compliance remediation project:
The initial engagement is a no-cost architecture review. In 90 minutes, Ideas2IT’s FDEs produce a written map of your current system against your compliance surface, identify the specific gaps driving your current friction, and give you a clear recommendation on path and scope. Teams evaluating custom LIMS development can review Ideas2IT’s healthcare software engineering practice before booking a session.
If your LIMS handles the basics but runs up a professional services bill every time your workflows change, surfaces compliance findings on things you thought were configured, or produces data your analytics team cannot use without heavy preprocessing, the architecture debt is already there. Every quarter that decision waits, the remediation scope grows.
In a 90-minute architecture review with Ideas2IT, you receive:
Schedule your LIMS architecture review
Didn't find what you were looking for?