You have raised the round. The product direction is clear. Now you need engineers who understand healthcare, not engineers who have read about it. In Austin’s 2026 healthtech market, that distinction is harder to make than it should be.
Austin-area startups raised $7.19 billion in venture capital in 2025, a 64.8% increase over the prior year[1]. Nationally, AI-enabled digital health companies captured 54% of all digital health funding[2]. The capital is real. The clinical problems are real. What gets consistently underestimated is the engineering infrastructure required to convert a funded product vision into software that health systems will actually deploy.
Most healthtech founders discover this the hard way. They hire a development partner, ship an MVP, and then spend the next six months retrofitting the compliance architecture that should have been foundational. That pattern has a name: the Compliance Retrofit Trap. It is the single most expensive mistake in healthtech engineering, and it is almost entirely avoidable with the right partner and the right architectural decisions made in the first 30 days.
Founders evaluating healthcare software development companies in Austin face a fragmented landscape: local generalist shops, offshore firms offering speed at the expense of compliance depth, boutique agencies with clinical fluency but limited scale, and enterprise consultancies whose timelines and price tags don’t fit a post-Series A burn rate. The wrong choice doesn’t surface as a bad review or a missed deadline. It surfaces six months later as an architectural rework that compresses runway and stalls the product roadmap.
This guide covers what Austin healthtech founders are building in 2026, how long development actually takes, what it costs, how to evaluate the right build approach, how to choose a development partner, where AI fits in the engineering workflow, and the four decisions that determine whether your product reaches clinical deployment on schedule or stalls in retrofit.
The healthtech products coming out of Austin in 2026 cluster around five categories, each with distinct engineering requirements and regulatory surface areas. Understanding which category your product falls into determines the compliance architecture, integration scope, and partner profile you need.
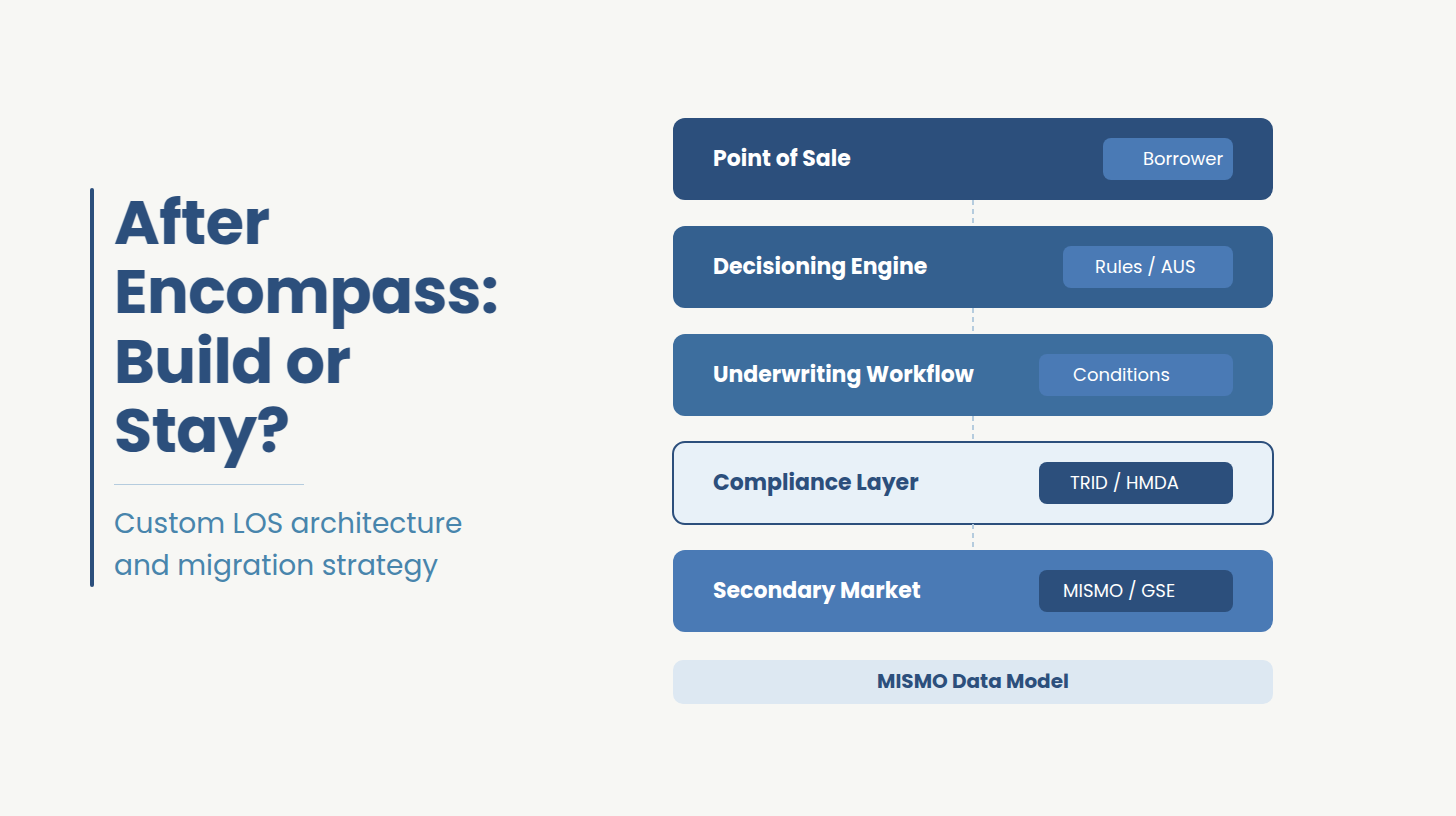
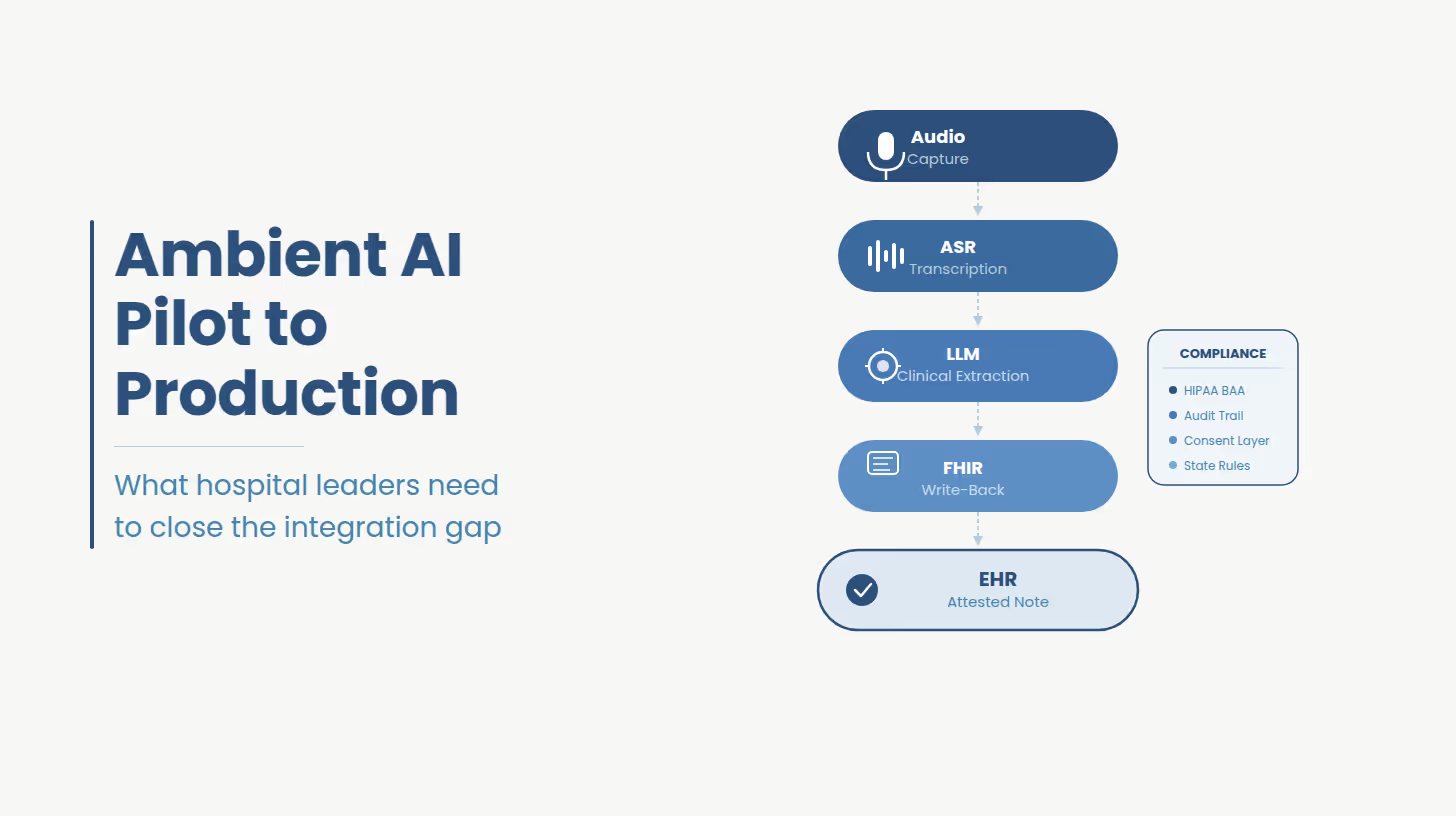
EHR-integrated clinical platforms remain the largest category. These are provider-facing and payer-facing systems that read from and write back to electronic health records. The technical requirement is bidirectional data exchange across multiple EHR vendors using FHIR and, in legacy environments, HL7v2. The commercial requirement is that health systems will not onboard a product that cannot talk to Epic, Cerner, or athenahealth on Day 1. This is the category where integration architecture makes or breaks the business model.
In Austin, companies like Findhelp have demonstrated the commercial scale possible when interoperability is architectural from the start.
AI-powered clinical documentation and decision support is the fastest-funded category nationally. AI-enabled companies captured 54% of all digital health funding in 2025[2]. Austin founders are building ambient documentation tools, clinical coding automation, and risk stratification engines. The engineering challenge is twofold: the AI model must perform in clinical settings, and every data pipeline that touches protected health information must be HIPAA-compliant by architecture, not by policy.
Austin-based founders are building in this category with backing from both local VCs and national digital health funds that tracked 54% of all 2025 digital health funding flowing to AI-enabled companies.
Remote patient monitoring and virtual care continues to expand, driven by CMS policy updates that have broadened reimbursement for home-based care delivery[3]. The engineering scope here includes device-agnostic data ingestion, real-time alerting, and integration with provider workflows. The regulatory scope includes FDA consideration if the software makes clinical recommendations based on patient-generated data.
Austin’s proximity to large health systems across Central Texas gives RPM founders direct access to pilot partners that most markets cannot match.
Claims automation and revenue cycle tools target the administrative burden that costs U.S. healthcare an estimated $30 billion annually in fragmented data alone[4]. Founders in this space are building AI-driven prior authorization, denial management, and payment reconciliation platforms. The integration surface area is wide: EHR systems, clearinghouses, payer portals, and billing engines.
Patient engagement and care navigation rounds out the landscape. These products sit between the provider and the patient, handling scheduling, care plan adherence, referral coordination, and outcomes tracking. The compliance requirement is lighter than clinical platforms but still substantial when PHI is in scope.
Each of these categories shares a common engineering dependency: the compliance, interoperability, and integration infrastructure must be architectural, not incremental. The category determines the scope. The architecture determines the timeline.
The honest answer is that healthcare software development takes longer than most founders budget for, and the variance is driven less by feature complexity than by three infrastructure variables that are routinely underestimated: EHR integration, compliance architecture, and approval pathways.
A clinical MVP with no EHR integration and a limited PHI footprint can reach a testable state in two to four months. This is the timeline for a standalone tool, a patient-facing app that does not exchange data with provider systems, or an internal analytics dashboard operating on de-identified data. The moment EHR integration enters scope, the timeline shifts materially. A startup that replaced its HL7 pipeline with a FHIR-based SMART gateway launched in four months instead of the projected seven, a 40% acceleration[5].
A full product with bidirectional EHR integration, HIPAA-compliant data infrastructure, and production-grade interoperability across multiple provider systems takes nine to eighteen months. The range is wide because the variables compound.
EHR integration is the largest timeline variable. The ranges below assume FHIR-first architecture from sprint one. HL7v2 legacy environments add 30–50% to each range.
Vendor certification adds four to eight additional weeks on top of development time. Epic’s App Orchard and Showroom process is the most demanding[6].
Building HIPAA into the data layer, encryption framework, audit trail system, and access control architecture from Day 0 adds four to eight weeks to the initial build. That is the cost of doing it right. The cost of doing it later is three to six months of rework after the MVP is already in testing, because compliance cannot be patched onto an architecture that was not designed for it. The gap between these two timelines is where the Compliance Retrofit Trap lives.
If the software qualifies as a Software as a Medical Device under FDA guidelines, the regulatory pathway adds months of documentation, testing, and review. ONC certification for EHR-facing products carries its own timeline. These are not optional steps that can be deferred without consequence. Health systems and payer organizations will not onboard a product that has not cleared the relevant approval gates, and every month spent waiting for approval post-build is a month of delayed contract revenue.
The founders who ship on schedule are not the ones with simpler products. They are the ones who scoped integration, compliance, and approvals as architectural commitments in the first engineering sprint, not as line items to be addressed before launch.
Cost ranges for healthcare software development are widely published and widely misleading. Most estimates quote development hours and hourly rates without accounting for the infrastructure costs that dominate regulated product builds. The numbers below reflect what Austin healthtech founders actually pay when compliance, interoperability, and integration are scoped honestly from the start.
A basic clinical MVP with no EHR integration, limited PHI handling, and a single-platform deployment runs $50,000 to $150,000. This covers core product engineering, a baseline HIPAA-compliant hosting environment, and initial QA. It does not cover the integration, compliance depth, or interoperability architecture that health system customers will require before signing a contract.
An MVP with a single EHR integration runs $100,000 to $250,000. The jump is not proportional to the feature count. It reflects the cost of building a FHIR-compliant data exchange layer, passing vendor certification, and standing up the audit and access control infrastructure that bidirectional clinical data exchange demands.
A full platform with multi-EHR interoperability, production-grade compliance architecture, and AI-powered clinical features runs $300,000 to over $1 million. The upper range applies to products operating across multiple EHR vendors, multiple payer systems, and multiple regulatory frameworks simultaneously.
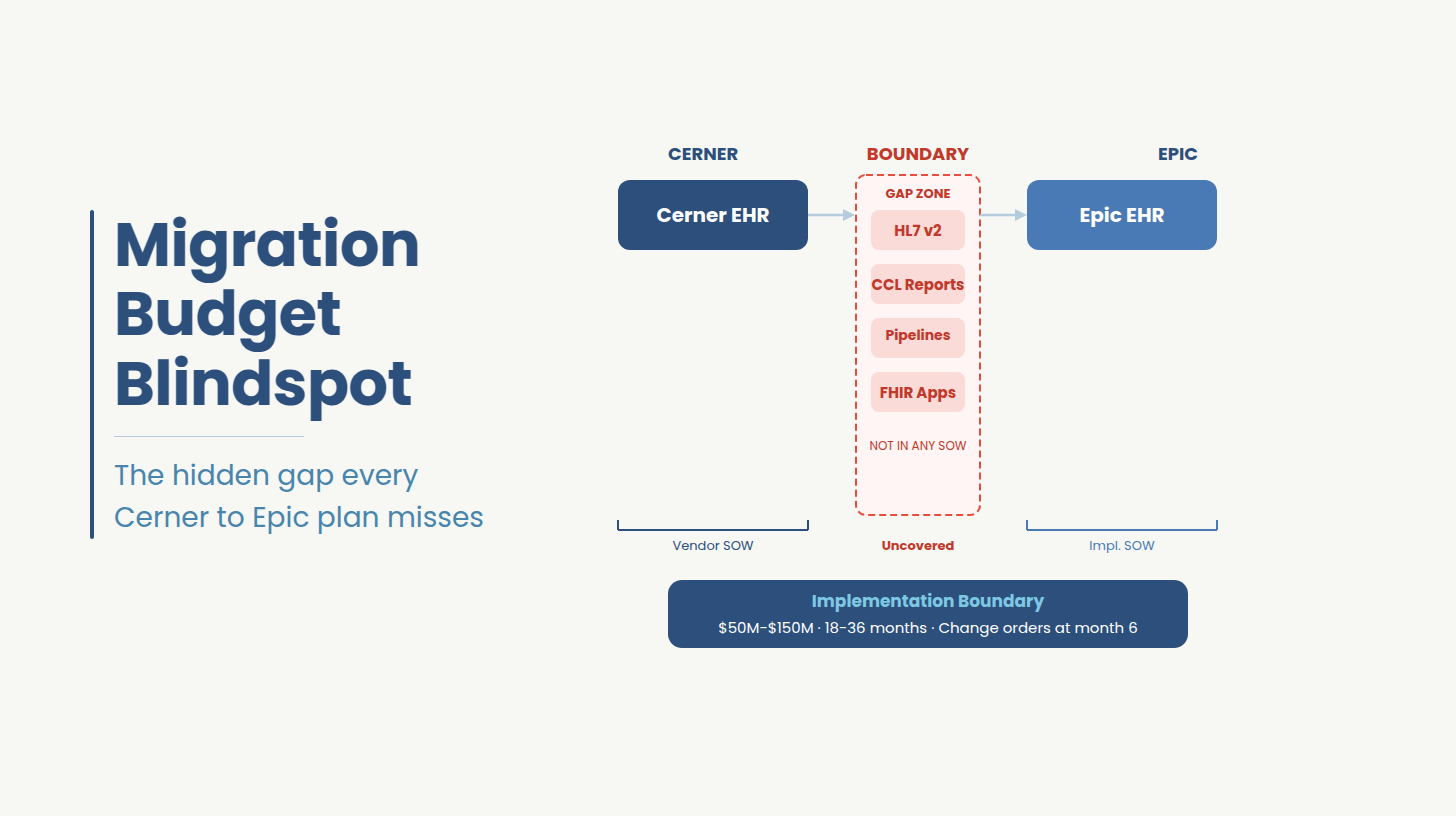
EHR integration is the cost category that surprises founders most frequently. A single read-only FHIR connection costs $15,000 to $30,000. Bidirectional integration with a single EHR vendor runs $30,000 to $80,000, with Epic at the high end due to App Orchard and Showroom certification requirements. A multi-platform integration suite exceeds $150,000. Ongoing maintenance costs $3,000 to $15,000 per interface per year for monitoring, error resolution, and vendor API version updates. Validation loops alone cost $10,000 to $20,000 per vendor[6][5].
HIPAA compliance cost is best understood as a ratio, not a line item. When compliance architecture is embedded from Day 0, it adds roughly 10 to 15 percent to the initial development budget. When compliance is deferred past the MVP and retrofitted onto an architecture that was not designed for it, the cost is 30 to 50 percent of the total project budget in rework, plus three to six months of engineering bandwidth consumed by remediation instead of product development. The financial argument for building compliance into the architecture from the first sprint is not philosophical. It is arithmetic.
The most expensive number in healthcare software development is not on any vendor’s pricing page. Healthcare data breaches cost an average of $9.77 million per incident, more than double the cross-industry average[7]. For a Series A startup, that figure is a terminal event.
Austin-based healthcare-specialized boutiques typically bill $150 to $220 per hour for senior engineers with FHIR and compliance depth. National enterprise healthcare IT firms run higher. Offshore firms offering healthcare development quote $40 to $80 per hour, with the tradeoff being compliance infrastructure that often requires domestic remediation before a health system security review.
The arithmetic is not always what it appears: a $60/hour offshore engagement that requires $80,000 in compliance rework before your first enterprise customer onboards is not cheaper than a $180/hour domestic engagement that builds compliance into the architecture on Day 0.
If your engineering roadmap does not include a compliance architecture layer, we can map one in a 60-minute working session. Just the blueprint your next board meeting needs.
Book the session →
The build approach a healthtech founder selects has consequences that outlast the first release. It determines how compliance is maintained as regulations evolve, how integration architecture scales as new health system customers onboard, and how engineering velocity holds up when the product roadmap gets more demanding after launch. There are three primary models, each with structural advantages and structural risks.
Building in-house offers maximum control over architecture, IP, and engineering culture. The founder sets the compliance posture, owns the integration decisions, and retains institutional knowledge inside the organization. For well-capitalized teams at Series B or later with the runway to invest in a six-to-twelve-month hiring cycle, in-house is the cleanest long-term path.
The constraint is talent. Demand for experienced healthcare software developers outpaces supply 2:1 in the US and Europe as of 2025. Healthcare-domain engineers who combine software engineering depth with fluency in clinical workflows, FHIR/HL7 interoperability, and HIPAA-compliant architecture are among the scarcest profiles in the market. CHIME’s annual surveys consistently identify the healthcare IT workforce gap as a top concern for industry leaders[8]. In Austin’s competitive engineering market, filling a single senior healthcare engineering role takes three to six months. Building a full team takes longer. For a post-Series A founder with 18 to 22 months of runway, that is not a planning inconvenience. It is a strategic risk that delays every downstream milestone.
Outsourcing to a development firm offers speed. A well-matched outsourcing partner with pre-built compliance infrastructure, established EHR vendor relationships, and healthcare-domain experience can compress the MVP timeline significantly. The founder trades some architectural control for faster time to market.
The risk is context loss. When the development team operates outside the founder’s engineering environment, building to a specification document rather than participating in the product’s daily decision-making, the output tends to be technically correct but architecturally disconnected. The code works in isolation. It does not account for the workflow assumptions, the data model decisions, or the compliance edge cases that only surface when engineers are embedded in the clinical problem. The result is rework at integration, rework at scale, or rework when the first health system customer’s security review surfaces gaps the spec did not anticipate. Outsourcing works when the partner has genuine healthcare depth and a delivery model that keeps their engineers close to the founder’s decision-making cadence. It fails when the engagement is transactional.
The third model puts engineers inside your engineering environment from Day 0, not alongside it. They work in your stack, attend your standups, align to your OKRs, and participate in the architectural decisions that determine the product’s compliance posture and integration ceiling. They are not contractors fulfilling tickets against a specification. They are engineering team members who bring healthcare-domain expertise, compliance architecture fluency, and integration experience that your existing team does not yet have.
This model addresses the two constraints that make in-house and outsourcing difficult for post-raise healthtech founders. It eliminates the hiring timeline of in-house by providing domain-specialized engineers immediately. It eliminates the context gap of outsourcing by embedding those engineers inside the product’s engineering culture from Day 0. The tradeoff is that the founder must invest in onboarding and integration the same way they would with a full-time hire, because the model only works when the embedded engineers operate as genuine team members, not as an external delivery function.
For Austin healthtech founders who have raised a Series A, have a product direction, and need healthcare-domain engineering depth they cannot recruit fast enough to meet their milestone commitments, the embedded model resolves the highest-risk variable in the build decision: time to qualified engineering capacity.
Austin’s healthcare software development landscape includes firms across a wide spectrum of size, specialization, and delivery model. For a healthtech founder evaluating partners, the useful distinction is not which company ranks highest on a directory listing. It is which category of firm matches the engineering requirements, compliance surface area, and stage of the product being built.
The landscape breaks down into four categories. Each serves a different founder profile, and choosing the wrong category is more costly than choosing the wrong firm within the right category.
Serve large provider networks, hospital systems, and payer organizations. Their engagement models are built for organizations with dedicated IT departments, procurement cycles, and change management processes. Engagements typically start in the six figures and extend over quarters, not weeks. Choose this category if you are a health system or a growth-stage company with enterprise-scale infrastructure needs and the budget to support a long engagement cycle.
The strongest match for founders who need clinical domain expertise at startup speed. Their engineers tend to have direct experience with HIPAA-compliant architectures, FHIR and HL7 integration, and the clinical workflow nuances that generalist developers miss. The risk with boutiques is ceiling: a firm with 15 to 40 engineers can deliver an MVP and support early-stage scaling, but may not have the platform infrastructure or team depth to sustain velocity through multi-EHR integration, AI feature development, and compliance expansion simultaneously.
The most common category in Austin’s development landscape and the most common source of mismatched healthtech engagements. Their strength is speed and flexibility; their gap is domain depth. A generalist firm may understand API development and cloud architecture but lack fluency in FHIR resource mapping, HIPAA audit trail design, or vendor certification processes. If your product touches clinical data, patient records, or payer systems, a generalist firm is a category mismatch regardless of their portfolio quality.
Platform-led engineering companies combine healthcare-domain depth with proprietary tooling that accelerates delivery structurally (automated discovery, AI-powered QA, code intelligence) rather than relying solely on individual engineer throughput. The delivery model is embedded: engineers operate inside the founder’s environment, not alongside it. This category is less common than boutiques or generalists and is typically identified through referral rather than directory search.
Offer the lowest cost and highest flexibility for pre-seed founders validating a concept. The risk is structural: freelancers operate without the compliance infrastructure, QA systems, and institutional knowledge that regulated product development requires. Choose this category for pre-seed validation, non-clinical prototyping, or supplementary feature work on a product whose core architecture was built by a team with healthcare-domain infrastructure.
What they do best: AI-powered healthcare app development with production-grade Epic and athenahealth integration, including SMART on FHIR implementation and App Orchard certification.
The tradeoff: Team size caps delivery capacity on simultaneous multi-EHR integration and large-scale compliance expansion.
Right fit when: You are building an AI-augmented clinical tool that needs EHR integration and HIPAA-compliant architecture without a separate compliance consultant.
What they do best: Deep, long-standing EHR integration across Epic, Oracle Health, Allscripts, and athenahealth, with active developer program memberships and a published EHR Integration Cost Guide.
The tradeoff: Austin-regional focus may limit scaling if your customer base extends to national health systems beyond Central Texas.
Right fit when: You need an Austin-based firm with established multi-vendor EHR relationships and a track record of working with both providers and digital health startups in the Central Texas market.
What they do best: Fully US-based healthcare development with senior engineers who have direct experience navigating HIPAA, ICD-10, HL7, and clinical data handling requirements.
The tradeoff: Smaller team size means capacity constraints on engagements that require parallel workstreams across integration, AI features, and compliance expansion.
Right fit when: You prioritize a domestic team with regulatory fluency and strong UX design within compliant architectures.
What they do best: Flexible team scaling with a mix of onshore strategy and offshore engineering capacity, including AI-native roadmap development for healthcare organizations.
The tradeoff: Healthcare is one vertical among several; deep clinical workflow and compliance infrastructure requires supplemental specialist oversight.
Right fit when: Your product’s healthcare regulatory surface area is manageable and you need flexible scaling with distributed engineering teams.
Disclosure: Ideas2IT is our company. It appears in this list because the framework this guide has laid out is what it was built to deliver. The reader can weigh that against everything else in this guide.
What they do best: Platform-led AI and software engineering with 800+ engineers, Forward Deployed Engineers who embed inside your stack from Day 0, and proprietary acceleration infrastructure (automated discovery, AI-powered QA, code intelligence, agentic migration) backed by SOC 2 Type II, ISO 27001, HIPAA, and AWS Healthcare Competency certifications.
The tradeoff: The embedded model requires genuine onboarding investment; it does not work as a hands-off outsourcing arrangement.
Right fit when: Your product requires healthcare-grade compliance architecture, multi-EHR integration, and AI-capable engineering at startup speed, and you need embedded domain expertise operating inside your engineering cadence from Day 0.
Choosing a healthcare software development partner is not a procurement decision. It is an architectural decision that determines whether the product’s compliance posture, integration capacity, and engineering velocity hold up under the conditions that matter most: a health system security review, a second EHR vendor integration, a board meeting where the CTO has to explain why velocity dropped after launch.
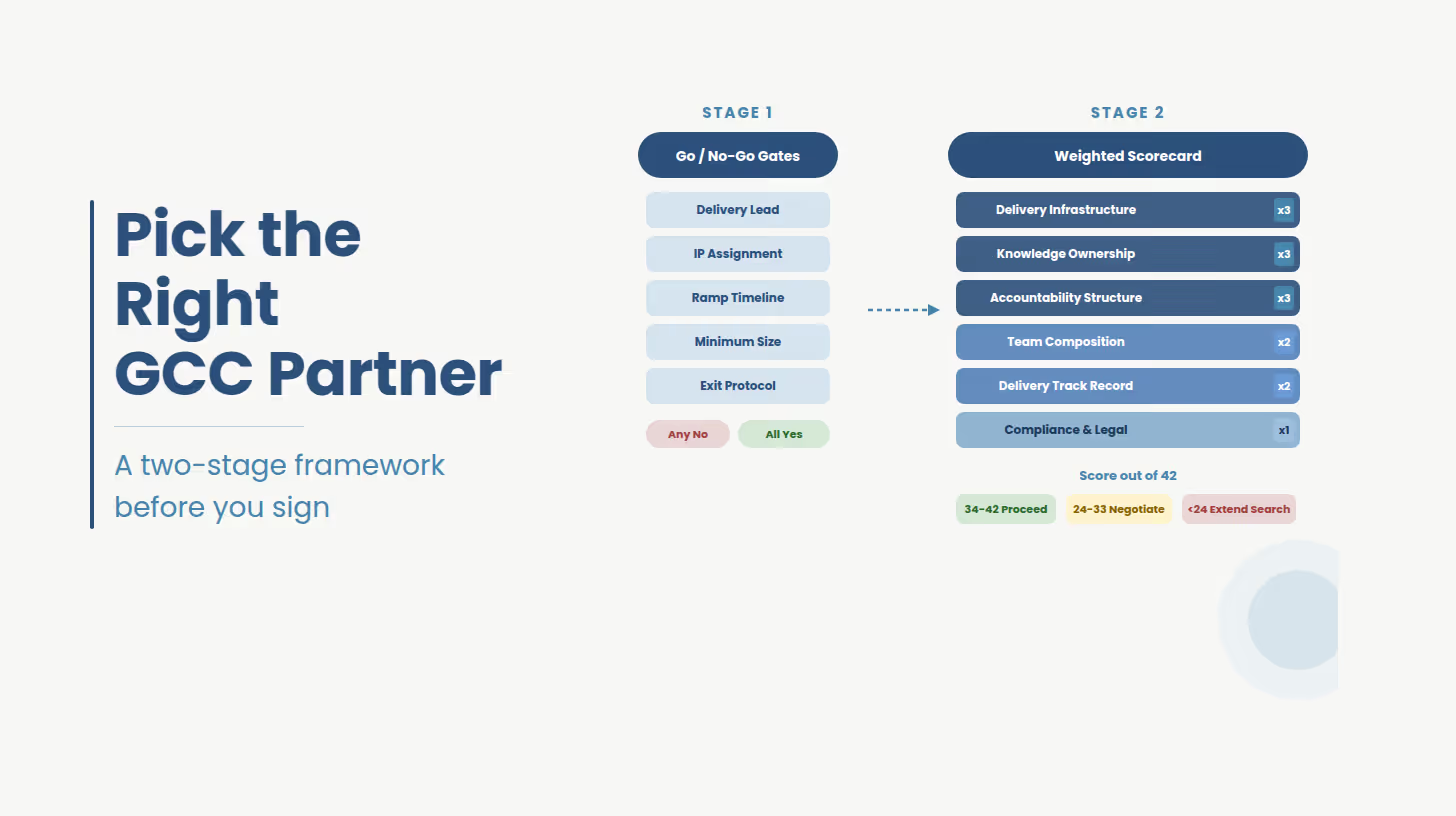
Five evaluation criteria separate partners who can deliver regulated healthcare software from partners who can build software that happens to be used in healthcare.
Every development firm’s website says HIPAA-compliant. The question that reveals depth is not whether they comply but how they architect compliance. Ask where encryption is implemented in the data layer. Ask how audit trails are structured. Ask how role-based access control is enforced across the application, not just at the login screen. Ask to see a previous HIPAA architecture diagram, not a certification badge. A firm that has built compliant healthcare systems will produce this artifact in minutes. A firm that treats compliance as a checklist will deflect toward their SOC 2 certificate and change the subject.
The relevant question is not whether the firm can integrate with Epic. It is how many production-grade Epic integrations they have maintained through App Orchard certification and API version updates. Ask how many EHR platforms they have integrated with in live clinical environments. Ask whether they hold active developer program memberships with Epic, Oracle Health, athenahealth, or other vendors relevant to your customer base. Ask what their average timeline has been for bidirectional integration, and whether that timeline included or excluded vendor certification. A firm with genuine integration depth will answer with specific numbers and specific constraints.
The question is whether their engineers will operate inside your engineering environment or alongside it. Inside means your stack, your standups, your sprint cadence, your OKRs. Alongside means a separate team delivering code against a specification, with sync meetings and handoff documents bridging the gap. Both models can produce working software. Only the embedded model produces software that reflects the architectural decisions, clinical assumptions, and compliance edge cases that surface in daily engineering work and never make it into a spec document.
A firm can be interested in healthcare without having engineers who understand it. The test is conversational. Ask their senior engineer to explain how FHIR resource mapping works for a bidirectional patient data exchange. Ask how they would structure an audit trail for a clinical decision support tool that writes recommendations back to the EHR. Ask what the compliance implications are when a patient’s PHI is processed by a third-party AI model. Engineers with healthcare-domain depth will engage these questions with specificity.
Portfolio screenshots and client logos are not proof. Ask for a specific engagement with a regulated health platform. Ask for the team size, the timeline, the integration scope, the compliance certifications maintained during the engagement, and the measurable outcome. A firm that has delivered healthcare software at scale will describe the engagement with the granularity of someone who lived it.
Red flags that signal a firm is not actually healthcare-specialized:
None of these are healthcare engineering partners. They are software firms that have completed one healthcare-adjacent project.
Not sure how your current shortlist holds up against these criteria? We run a 60-minute architecture assessment for Austin healthtech founders who have raised capital and are making build decisions now. The output is a documented compliance and integration architecture recommendation.
Book the assessment →
AI in healthcare software development is discussed most often as a product feature: clinical decision support, diagnostic imaging, predictive risk scoring. Those are valid product applications. But for a healthtech founder making engineering decisions in 2026, the more immediately consequential question is where AI fits in the development workflow itself, not just in the product that gets shipped.
Four applications are reshaping how healthcare software is engineered, tested, documented, and deployed. Each is production-ready today, not theoretical.
Ambient listening tools that generate SOAP notes, after-visit summaries, and structured clinical data from provider-patient conversations have proven the model at scale. Several companies in this space reached unicorn valuations in 2025 on the strength of 85% adoption rates and measurable reductions in clinician documentation time[2]. For founders building in this category, the engineering requirement is an NLP pipeline that handles protected health information compliantly from ingestion through storage, with encryption, access control, and audit infrastructure embedded in the data flow rather than applied as a post-processing layer.
Manual test case creation for healthcare software is slow and error-prone. Clinical workflows have branching logic, role-based access conditions, and compliance validation requirements that multiply the test surface area far beyond what a typical SaaS product demands. AI-native QA tools that auto-generate 60 to 70 percent of test cases from clinical workflow definitions compress QA cycles while maintaining the compliance coverage that health system security reviews require. Engineering teams adopting this approach report doubling QA velocity without increasing headcount. For a post-Series A founder, that is the difference between a quarterly release cycle and a monthly one.
As healthcare products scale, the codebase grows, the team changes, and the architectural decisions that determined the compliance posture six months ago are no longer legible to the engineers working on the product today. AI-powered code intelligence tools that document architectural decisions, flag compliance gaps during code review, and generate contextual documentation for regulated codebases reduce the institutional knowledge risk that healthcare startups carry as they grow. A new engineer joining the team can understand the compliance architecture of the codebase in days rather than weeks.
Manual discovery of a legacy system’s data model, integration points, and compliance surface area takes six to eight weeks of senior engineering time. AI-powered assessment tools that automate the discovery process compress that timeline to days, producing a structured map of the system’s architecture, data flows, and integration dependencies. For founders whose products must connect to hospital systems built on decades-old infrastructure, automated discovery eliminates the most unpredictable variable in the project timeline.
These four applications share a common characteristic. They do not replace the healthcare-domain engineer. They multiply the output of a team that already has domain depth. The tools are powerful. They require qualified operators.
The moment a third-party AI model processes protected health information, the compliance surface area expands in ways that most development teams do not anticipate. A Business Associate Agreement must be in place with every AI vendor whose model touches PHI, including the foundation model provider. The data pipeline from ingestion through the model and back to storage must maintain encryption, access control, and audit trail continuity. De-identification is not a workaround: if the data can be re-identified in context, it is PHI regardless of how it was preprocessed before reaching the model.
The practical requirements for HIPAA-compliant AI implementation:
BAA in place with every third-party model provider before data touches the model. PHI never sent to a model endpoint that logs inputs by default; confirm logging settings with each vendor. Encryption in transit and at rest maintained through the entire AI data pipeline, not just at the application layer. Audit trail capturing what data was sent, when, under whose authorization, and what was returned. Access control enforced at the pipeline level.
The proposed 2025 HIPAA Security Rule updates, with a final rule anticipated from HHS in 2026, are specifically expanding requirements around AI system governance and risk analysis documentation. Founders building AI features today need to architect for those requirements now, not retrofit for them after the rule takes effect.
Every healthtech product that reaches clinical deployment passes through four architectural decision points. Each has a right path and a wrong path. The wrong path is almost always the one that feels faster at the time and costs more by the time the product reaches its first health system customer.
These are not product decisions. They are engineering infrastructure decisions. They are made in the first 30 days of development and they determine the trajectory of the next 18 months.
The most common mistake in healthtech engineering is treating HIPAA compliance as a pre-launch requirement rather than a foundational architecture decision. This is the Compliance Retrofit Trap. When compliance is deferred, the data layer gets designed without encryption architecture. The access control framework gets stubbed out with placeholder logic. The audit trail gets scoped as a logging feature rather than a compliance system. The team ships faster in the first three months. Then a health system security review surfaces the gaps.
Building compliance architecture from Day 0 adds 10 to 15 percent to the initial development budget. Retrofitting it after the MVP adds 30 to 50 percent of the total project cost in rework, plus three to six months of engineering time that was budgeted for product development. The median VC-backed startup that fails does so within 22 months of its last raise[9]. Three to six months of compliance rework is not a delay. It is a material reduction in the company’s survival window.
The product roadmap says “Epic integration” with a two-week estimate and a single engineer assigned. The reality is that EHR integration is a system-level commitment that determines data architecture, API design, authentication flows, and vendor relationship management for the life of the product.
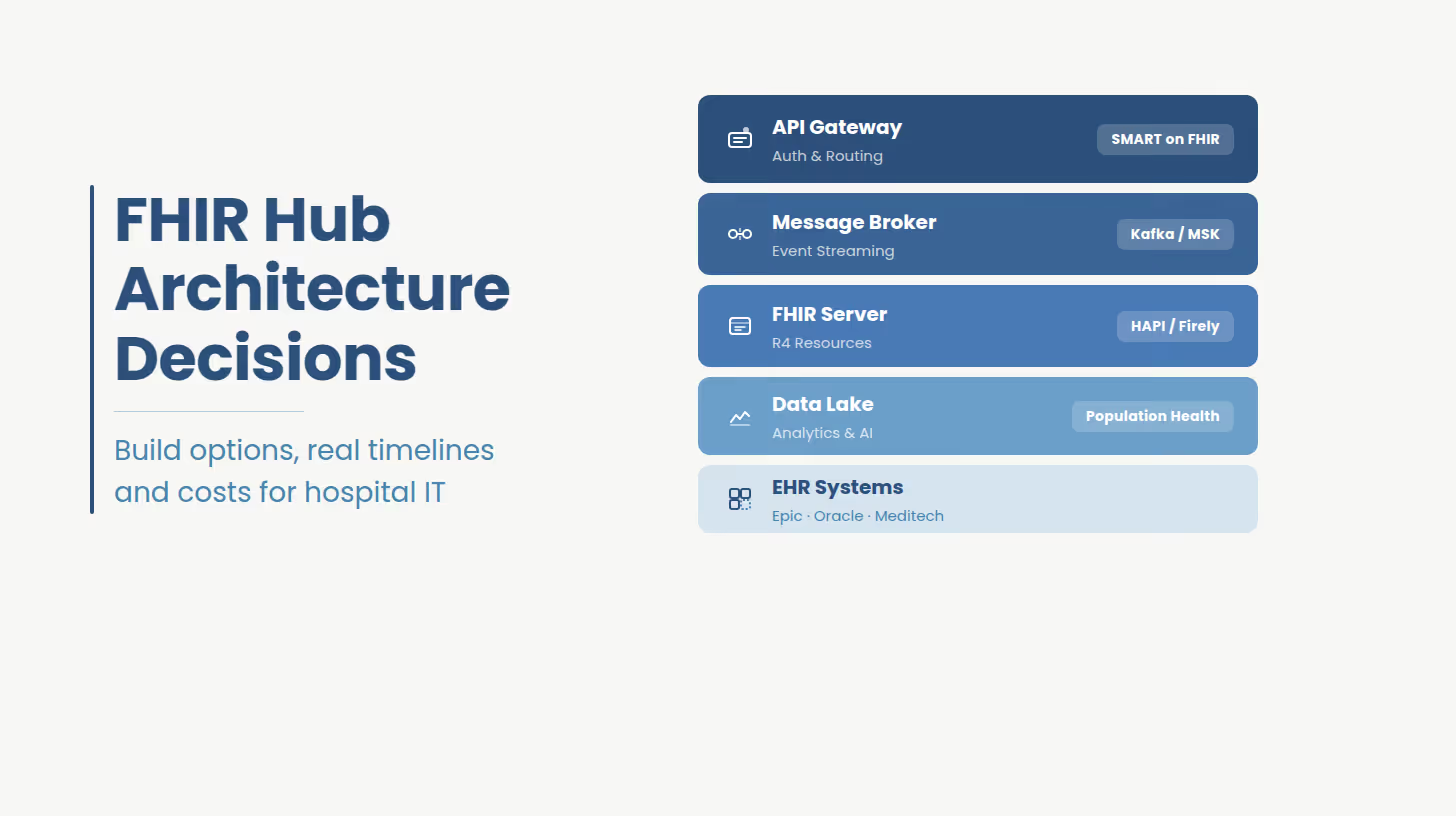
Founders who scope integration as a feature build one-off connectors for each EHR vendor. Each connector has its own data mapping, its own authentication logic, its own error handling. The second integration doubles the maintenance surface. The third makes it unmanageable. Founders who scope integration as a system invest in FHIR-first architecture from the first sprint. A standardized resource mapping layer handles data exchange across vendors. A centralized authentication framework manages SMART on FHIR and OAuth2 flows once, not per vendor. The per-customer integration cost drops with each new health system because the architecture was designed for portability.
The engineers who design the compliance layer, scope the integration architecture, and build the clinical data pipelines in the first 90 days are making decisions that constrain or enable every engineer who works on the product afterward. When those engineers lack healthcare-domain fluency, the decisions they make will be technically reasonable and clinically uninformed.
The specific gaps that surface most often when the first 90 days are staffed without healthcare-domain depth: data models that do not account for FHIR resource versioning, audit trail designs that satisfy logging requirements but fail access control audits, authentication flows that work for the first EHR vendor and break for the second, and AI pipelines that process PHI without BAA coverage because the engineer did not know to ask whether the model provider required one.
None of these gaps are obvious during development. All of them are obvious during a health system security review. The cost of finding them there instead of in sprint two is measured in months of rework.
Quality assurance in healthcare software is not a velocity tax. It is a compliance requirement. Every clinical workflow, every data exchange pathway, every access control rule must be tested against regulatory requirements, not just functional requirements. The test surface area in a HIPAA-compliant, EHR-integrated product is an order of magnitude larger than in a standard SaaS application.
Manual QA in this environment is slow, inconsistent, and fragile. Test cases are written by hand, executed by hand, and maintained by hand. When the product evolves, the test suite lags behind. Compliance gaps accumulate silently until an audit or a security review forces the team to reconcile months of untested changes.
AI-native QA tools in production healthcare environments auto-generate 60 to 70 percent of test cases from clinical workflow definitions. In Ideas2IT’s healthcare engagements, this approach has doubled QA velocity while maintaining the compliance coverage that health system security reviews require. The release cycle compresses from quarterly to monthly. For a healthtech founder operating on a finite runway, that acceleration is measured directly in the number of product iterations that fit inside the fundraise window.
Ideas2IT Technologies is a platform-led AI and software engineering company with 800+ engineers, founded in 2009 and headquartered in Plano, Texas. Healthcare clients include Medtronic and Mayo Clinic. Certifications include SOC 2 Type II, ISO 27001, HIPAA, and AWS Healthcare Competency.
The delivery model is Forward Deployed Engineers: engineers who embed inside the founder’s stack, standups, and OKRs from Day 0, not contractors delivering against a specification document. The platform infrastructure behind them (automated discovery, AI-powered code intelligence, QA automation, and agentic data migration) addresses each of the four engineering decisions in this guide structurally, not individually.
For Austin healthtech founders who have raised capital and need healthcare-domain engineering depth operating inside their engineering environment from the first sprint, that combination is what the Ideas2IT's Healthcare engagement is built to deliver.
The Compliance Retrofit Trap is expensive because it is discovered late. The architecture assessment that prevents it takes 60 minutes.
Ideas2IT runs a $0 Healthtech Architecture Assessment for Austin-area healthtech founders who have raised capital and are making engineering decisions that will determine whether their product reaches clinical deployment on schedule or stalls in retrofit.
The session covers three things. First, a compliance architecture audit of the founder’s current engineering roadmap, identifying where HIPAA, SOC 2, and data handling requirements are embedded in the architecture and where they are deferred. Second, an integration scope assessment: which EHR platforms, what data exchange requirements, what vendor certification pathways, and what the realistic timeline looks like when integration is scoped as a system rather than a feature. Third, an identification of Compliance Retrofit Trap indicators in the existing plan, the specific architectural decisions that, if left unaddressed, will surface as rework in six to nine months.
The output is a documented architecture recommendation. A technical artifact the founder can take to their next board meeting, use to evaluate any engineering partner, or hand to their internal team as a compliance architecture blueprint.
If your product touches clinical data, integrates with EHR systems, or operates under HIPAA, and your engineering roadmap does not yet include a compliance architecture layer, this session will tell you exactly where the gaps are and what it takes to close them before they become expensive.
[1] Crunchbase, “Austin’s Star Is Still Shining Bright: Venture Funding To City’s Startups Hits All-Time High” https://news.crunchbase.com/venture/all-time-high-funding-to-austin-startups-2025-ai-robotics-manufacturing/
[2] Rock Health, “2025 Year-End Digital Health Funding Overview” (via Navitize) https://learn.navitize.com/blog/invest/digital-health-startups-2026
[3] Taction Software, “EHR Integration Cost Guide 2026” https://www.tactionsoft.com/ehr-integration-cost-guide/
[4] CB Insights, “Why Startups Fail: Top 9 Reasons” https://www.cbinsights.com/research/report/startup-failure-reasons-top/
[5] IBM / Ponemon Institute, “Cost of a Data Breach Report 2024” (via Sidebench) https://sidebench.com/most-common-health-tech-challenges/
Didn't find what you were looking for?